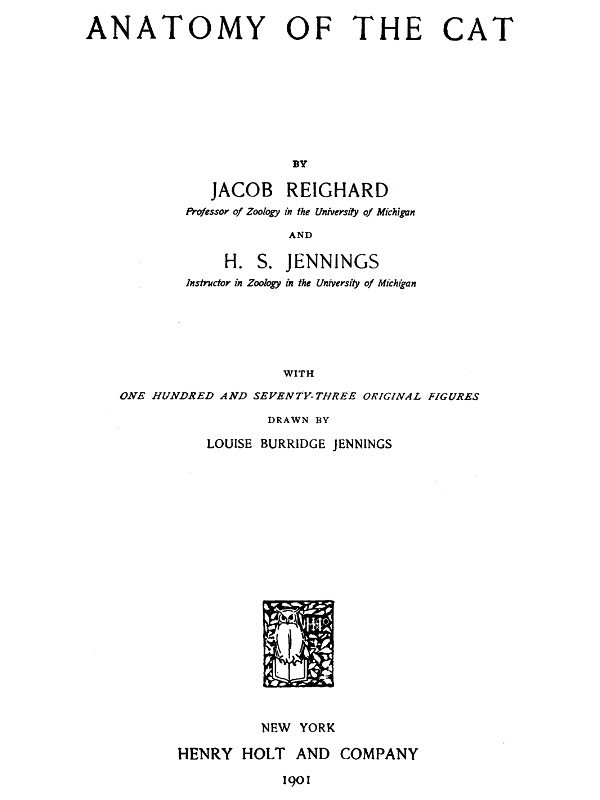
Fig. 114.—Muscles of the Anus and Urogenital Organs in the Female.
a, M. sphincter ani externus; b, M. levator vulvæ; c, M. sphincter ani internus; d, M. constrictor vestibuli; e, M. ischiocavernosus (cut); f, M. urethralis; g, M. caudoanalis; h, M. caudovaginalis; i, M. transversus perinei; j, M. caudorectalis. 1, the tail; 2, anus; 3, vulva; 4, rectum; 5, vagina; 6, neck of the bladder.
Origin from the sides of the sphincter ani internus (c). The muscle forms a distinct bundle two or three millimeters wide, which passes ventrocaudad and is inserted into the ventral surface of the urogenital sinus, caudad of the insertion of the ischiocavernosus (e).
M. caudovaginalis (Strauss-Durckheim) (h).—A slender band just craniad of the caudoanalis (g), and corresponding to the caudocavernosus of the male.
Origin from the median line of the ventral surface of the first two caudal vertebræ. The muscle passes caudoventrad, lying between the levator ani and the caudorectal (j), and is inserted into the ventral side of the urogenital sinus, at the base of the clitoris.
M. urethralis (f).—This consists of fibres surrounding the cranial part of the urogenital sinus and the caudal parts of the vagina and neck of the bladder.
Origin partly on the caudal part of the symphysis of the ischium, partly from the ventral surface of the urogenital sinus, where the fibres are attached to the corpora cavernosa clitoridis. The fibres pass dorsad over the surface of the sinus, and over the surface of the union of the vagina and neck of the bladder, to be inserted into the sides of the vagina and the dorsal surface of the urogenital sinus.
THE CIRCULATORY SYSTEM.
I. THE HEART. COR.
The heart lies in the mediastinum, enclosed in the pericardial sac, and projects rather more toward the left than toward the right. It is an ovoid or pear-shaped organ, with its long axis directed approximately craniocaudad. Its caudal end or apex is, however, directed slightly ventrad and to the left, while the larger cranial end or base faces slightly dorsad as well as craniad.
Laterally and dorsally the heart is largely covered by the lungs. The ventral side and a considerable portion of the lateral surface are, however, not thus covered, so that they lie against the thoracic wall. The heart extends from about the fourth or the fifth to the eighth rib, and its apex touches the diaphragm.
The cavity of the heart is divided by a longitudinal dorsoventral septum into lateral halves—a right and a left side. Each side is again divided by a transverse dorsoventral septum (auriculoventricular) into two chambers, one of which, the auricle, lies at the base; the other, the ventricle, lies at the apex of the heart. There are thus right and left auricles and right and left ventricles. An external groove, partly filled with fat, separates the auricular portion of the heart from the ventricular part; this groove is known as the sulcus coronarius.
Each auricle or ventricle has a single set of blood-vessels either leaving it or entering it. Thus the blood enters the right auricle by the inferior and superior venæ cavæ (Fig. 116, d and e) (præcava and postcava). It passes thence into the right ventricle, and from the right ventricle to the lungs by a single pulmonary artery (Fig. 115, f). It returns to the left auricle by the numerous pulmonary veins (Fig. 116, g, h, i), and passes thence to the left ventricle. From the left ventricle it passes to the body by a single aorta (Fig. 115, g).
When the heart is viewed from the ventral surface (Fig. 115), a considerable blood-vessel, the coronary artery (q), running from the base to a point a little to the right of the apex, indicates the position of the septum (ventricular septum), between the right (a) and left (b) ventricles. The apex thus belongs to the left ventricle. From the cranial end of the right ventricle the pulmonary artery (f) is seen passing obliquely craniad and toward the left. Beneath the pulmonary artery the aorta (g) appears rising from the middle of the base of the heart and passing directly craniad. At the base appears a part of the auricular appendage of the left auricle (d), and at the right a part of the right auricular appendage (c). The former (d) is larger and bent at right angles, so that its free end is directed toward the apex.
In the dorsal view (Fig. 116) the position of the ventricular septum is not indicated. On the surface of the left ventricle a short distance from the ventricular septum and nearly parallel to it are seen branches of the coronary artery and the coronary vein passing toward the apex. Craniad of the left ventricle is seen the left auricle (b) with the pulmonary veins (g, h, i) opening into it. Craniad of the right ventricle (a) is the right auricle (c) with the venæ cavæ (d and e) opening into it near the middle. Coming from beneath the auricles are seen the pulmonary artery (j) and the aorta (f).
The chambers of the heart.
1. The right auricle (atrium dextrum) (Figs. 115 and 116, c). Externally the right end of the right auricle projects so as to form its auricular appendage (Fig. 115, c) which lies at the right of the base of the aorta (Fig. 115, g). The superior vena cava (Fig. 116, e) is seen entering near the cranial end of the auricular septum opposite the base of the aorta. The inferior vena cava (Fig. 116, d) enters the auricle near the coronary sinus and close to the auricular septum. The netted appearance which the wall, especially that of the appendage, presents externally is due to the muscular thickenings of the wall (musculi pectinati).
Fig. 115.—a, right ventricle; b, left ventricle; c, right auricular appendage; d, left auricular appendage; e, conus arteriosus; f, pulmonary artery; g, aortic arch; h, thoracic aorta; i, vena cava superior; j, innominate artery; k, left subclavian artery; l, left common carotid; m, right common carotid; n, right subclavian; o, azygos vein; p, the two innominate veins; q, coronary artery.
Fig. 116.—a, right ventricle; b, left auricle; c, right auricle; d, vena cava inferior; e, vena cava superior; f, aorta; g, h, i, groups of pulmonary veins (g, dorsal group; h, sinistral group; i, dextral group); j, pulmonary artery (division into two); k, innominate artery; l, left subclavian; m, left common carotid; n, right common carotid; o, right subclavian; p, azygos vein.
The cavity (including that of the auricular appendage) is somewhat egg-shaped, with its long axis transverse. The musculi pectinati, which branch and unite into a network, are most abundant on its dorsal wall at the right. The axes of the two venæ cavæ if produced into the cavity of the auricle would meet one another at its centre and nearly at right angles. Caudad of the opening of the inferior vena cava is seen the slit-like opening of the coronary sinus, guarded craniad by the semilunar valve of the coronary sinus (or valve of Thebesius). The coronary sinus receives blood from coronary veins, which collect it from the walls of the heart.
In the auricular septum ventrad of the opening of the inferior vena cava is seen a faintly marked smooth oval depression, the fossa ovalis. When the auricular septum is examined by transmitted light it is seen to be thinner over the fossa ovalis. There is an opening, foramen ovale, at this point in fœtal life, so that the blood of the inferior vena cava then passes directly from the right auricle to the left auricle. Caudad the cavity of the right auricle communicates with that of the ventricle by the large oval auriculoventricular opening, which is guarded by the tricuspid valves (Fig. 117).
2. The right ventricle (ventriculus dexter) (Figs. 115 and 116, a) does not reach quite to the apex of the heart, so that it makes up less than one-half of its ventricular portion. It makes a half-spiral turn about the left ventricle, from its lateral side at the apex toward its ventral side at the base, where it ends in the pulmonary artery (Fig. 115, e). Its wall is very thin as compared with that of the left ventricle. Its cavity (Fig. 117) is nearly flat on its medial side, convex on its lateral side. It communicates with the auricle craniodorsad. Cranioventrad the cavity is narrower and turns around toward the ventral side of the heart and opens into the pulmonary artery. That portion of the ventricle between the auriculoventricular opening and the pulmonary artery is the conus arteriosus (Fig. 115, e; Fig. 117, f). Internally the wall presents many muscular trabeculæ (Fig. 117, a) of various sizes. These are more numerous over the ventricular wall than on the septum. They do not occur on the conus (f). Surrounding the auriculoventricular opening is the tricuspid valve (Fig. 117, d, d′, d″). It consists of three flaps. One of these (d′) is septal (i.e., it lies against the septum), while of the two others which do not lie against the septum, one is dorsal (d″) and the other ventral. Each flap is thin, semicircular, and membranous, and is attached to the border of the auriculoventricular opening by the diameter of the semicircle. The free border of each is attached to the wall of the heart by numerous delicate tendinous bands, the chordæ tendineæ (c), some of which are attached to the lower face of each valve. The chordæ tendineæ of the septal valve (or most of them) are attached at their opposite ends to the septum directly, while those of the dorsal and ventral flaps are attached to the ends of three or more band-like muscles, columnæ (or trabeculæ) carneæ (b), which are fixed by their opposite ends to the ventricular wall.
Fig. 117.—Heart, with Right Ventricle laid open to show the Tricuspid Valve.
a, trabeculæ; b, columnæ carneæ; c, chordæ tendineæ; d, d′, d″, the three flaps of the tricuspid valve; e, aorta; f, conus arteriosus, laid open; g, semilunar valves of the pulmonary artery.
Between the conus arteriosus (f) and the pulmonary artery are three pocket-like semilunar valves (Fig. 117, g), one ventral, one dextral, and one sinistral. Between each valve and the wall of the pulmonary artery there is an enlargement of the cavity of the artery, one of the pulmonary sinuses (or sinuses of Valsalva). Beyond the sinuses the pulmonary artery divides into right and left branches (Fig. 116, j).
3. The left auricle (atrium sinistrum) (Fig. 115, d; Fig. 116, b). The auricular appendage (Fig. 115, d) is bent at right angles and its apex turned caudad. The cavity is thus irregular. Muscular trabeculæ occur only in the auricular appendage. When the auricular septum is examined by transmitted light the position of the fossa ovalis is indicated at about the middle of the septum as seen from the left side. Ventrad of it is a fold of the septal wall.
The pulmonary veins enter the dorsal wall of the auricle in three groups (Fig. 116, g, h, i). Each group opens into a more or less pronounced sinus or extension of the auricular cavity. The sinuses may be called, on account of their position, dorsal (g), sinistral (i), and dextral (h).
4. The left ventricle (Fig. 115, b) occupies rather more than the left half of the base of the heart. Its walls are two or three times as thick as those of the right ventricle. Internally its walls present a few muscular bands, comparable to the trabeculæ of the left ventricle. There are two very large columnæ carneæ, one dorsad and one ventrad. At the cranial end it communicates near the lateral wall with the left auricle by the auriculoventricular opening, and near the septum with the aorta. The bicuspid valve (or mitral valve), which guards the auriculoventricular opening, consists of two flaps, one septal and one lateral. Their chordæ tendineæ, which come from their free borders as well as from their outer surfaces, are attached to the columnæ carneæ, chordæ passing from both valves to each columna carnea.
The opening into the aorta is guarded by three aortic semilunar valves, each of which partly conceals an aortic sinus (or sinus of Valsalva). One valve is dorsal, one sinistral, and one dextral. In the dextral sinus is the opening of one of the coronary arteries, which carry blood to the walls of the heart.
Pericardium.
The pericardium is a sac enclosing the heart. It lies in the middle mediastinum, and the two halves of the mediastinal septum with their fat may be dissected away from it. Its wall is composed of two layers, an external firm fibrous layer and an internal layer of flattened epithelial cells similar to the peritoneal epithelium (serous layer). The fibrous layer forms a sac which repeats roughly the form of the heart. This sac is attached to the aorta at the point of origin of the subclavian artery, to the pulmonary artery at its bifurcation, and to the venæ cavæ and pulmonary veins near their entrance into the heart. At these points it is continuous with the fibrous coats of the vessels named, and from them it is reflected over the heart, forming a complete sac enclosing it but not attached to it anywhere. The heart lies within this sac. The serous layer lines the fibrous sac and gives to the surface of the heart and fibrous layer a smooth glistening appearance. It is reflected over the heart. The relation of the heart to it is much the same as the relation of the intestine to the peritoneal sac. The serous layer consists therefore of two portions, parietal, lining the sac, and visceral, covering the heart. The parietal and visceral portions are continuous along a line which runs approximately parallel to the auriculoventricular groove and encloses all the great blood-vessels. Within this line the heart lies against the fibrous layer of pericardium and is not covered by the serous layer. The serous layer is easily dissected free from the heart-wall, but its parietal portion is closely adherent to the fibrous layer.
II. THE ARTERIES. ARTERIÆ.
1. A. pulmonalis, the Pulmonary Artery
(Fig. 115, f).
The pulmonary artery passes craniodorsad and slightly to the left from the cranial end of the conus arteriosus. One to one and a half centimeters from the conus it divides into right and left branches (Fig. 116, j). Just before the division the dorsal surface of the pulmonary artery is connected by the short ligamentum arteriosum, or ligamentum Botalli, with the aorta. This is the remnant of a canal which in fœtal life forms a free communication between the pulmonary artery and the aorta; this canal is known as the ductus Botalli. The ligament is almost or quite obliterated in the adult cat.
The left branch of the pulmonary artery passes to the left lung, crossing ventrad of the thoracic aorta. It then divides into branches which pass to the lobes of the left lung. The point of division of the left branch of the pulmonary artery lies craniad of all the lobes of the lung, so that the lobes of the left lung are said to be all hyparterial, i.e., below (or caudad of) the artery.
The right branch passes under (dorsocaudad of) the aortic arch, and reaches the right lung at about the junction of the cranial lobe with the remainder of the lung. The cranial lobe of the right lung is therefore said to be eparterial, since it is craniad of the pulmonary artery; the other lobes are hyparterial. The right branch divides at its entrance to the lung and is distributed to its lobes.
2. Aorta
The aorta is the single great vessel which conveys blood from the left ventricle. It makes a sharp semicircular curve dorsad (Fig. 118, a′) and to the left, passes caudad at the left side of the vertebral column, and passes between the crura of the diaphragm to reach the abdominal cavity. It is divisible into thoracic aorta (Fig. 118) and abdominal aorta (Fig. 126).
A. Thoracic Aorta
(Fig. 118).—The first portion of the thoracic aorta, curved as above described, is the aortic arch (a′). It lies in the thoracic cavity opposite the interval between the third and fourth or fourth and fifth ribs. It is separated from the vertebral column on the right by the superior vena cava (q), and on the left by the œsophagus (4). At its beginning it lies a little to the right of the median plane; but it passes at once to the left side of the vertebral column.
Branches of the Thoracic Aorta.
1. Aa. coronariæ.—The coronary arteries are two. They arise from the aortic sinuses. The left one (Fig. 118, p) leaves the aorta on the left side, passes dorsad of the pulmonary artery, and divides into two branches, one of which follows the auriculoventricular groove (sulcus coronarius) to the dorsal side of the heart and sends branches to the adjacent heart-walls, while the other runs onto the ventricles, following approximately the ventral border of the ventricular septum. The right coronary artery passes in the auriculoventricular groove toward the right and dorsad, and supplies the adjacent walls of the heart.
2. A. anonyma (Fig. 115, j; Fig. 118, b).—The innominate artery passes craniad from the convexity of the aortic arch (a′). It gives rise first to a small mediastinal artery (m) which passes ventrad into the mediastinum, then to the left common carotid (Fig. 115, l), then to the right common carotid (Fig. 115, m). Sometimes the carotids are given off from a common trunk. Beyond the right common carotid the innominate is continued as the right subclavian (Fig. 115, n).
Fig. 118.—Vessels of the Thorax, Viewed from the Left Side.
a, aorta (a′, aortic arch); b, innominate artery; c, left subclavian; d, right subclavian; e, right common carotid; f, left common carotid; g, costocervical axis; g′, vertebral artery; h, internal mammary artery; i, axillary artery; j, thyrocervical axis; k, A. transversa scapulæ; m, mediastinal artery; n, intercostal arteries; o, œsophageal arteries; p, left coronary artery; q, superior vena cava; r, internal mammary vein; s, the two innominate veins; t, sternal artery; u, costocervical vein; v, vertebral vein; w, axillary vein; x, vein to clavotrapezius and lateral ends of the pectoral muscles; y, vein accompanying second branch of A. transversa scapulæ; z, thyrocervical vein. 1, external jugular vein; 2, internal jugular vein; 3, vena cordis magna; 4, œsophagus; 5, thoracic duct; 6, one of the lymphatic ducts from the neck. I, first rib (cut); VIII, eighth rib (cut); XII, twelfth rib (cut).
3. A. subclavia sinistra (Fig. 115, k; Fig. 118, c).—The left subclavian passes craniad from the convexity of the aortic arch. It curves about the first rib (Fig. 118, I) to enter the armpit, where it becomes the axillary artery (i).
4. Aa. intercostales (n).—The intercostal arteries are given off from the dorsal side of the aorta. Each passes to an intercostal space and divides into three branches. One of these passes ventrad along the caudal margin of the cranial one of the two ribs between which it extends. Another goes to the deep muscles of the back, and the third enters the spinal canal through the intervertebral foramen. The arteries for the first and second (and sometimes the third) intercostal space usually arise from the subclavian (costocervical axis, Fig. 118, g).
5. Aa. bronchiales.—The bronchial arteries are two, and arise either from the aorta opposite the fourth intercostal space or from the fourth intercostal arteries. They accompany the bronchi to the lungs.
6. Aa. œsophageæ (Fig. 118, o).—The œsophageal arteries are small branches of varying origin passing to the œsophagus.
7. Aa. lumbales.—The lumbar arteries correspond to the intercostals, but pass off between the lumbar vertebræ. The obliquity of the diaphragm throws the origin of one or two pairs of them within the thorax.
A. carotis communis. The Common Carotid Artery.
(Fig. 115, l and m; Fig. 119, a).
The two common carotid arteries arise from the innominate artery in the manner already described. Each passes craniad along the side of the trachea. In the thorax (Fig. 118, f) the common carotid lies mediad of the subclavian artery (Fig. 118, c) and dorsad of the superior vena cava (Fig. 118, q). In the neck (Fig. 119) the artery lies, accompanied by the vagus and sympathetic nerves and the internal jugular vein (b), in the space between the longus capitis muscle (7) and the trachea (14); it is covered ventrally by the sternomastoid and sternothyroid (2) muscles, lying close to the lateral border of the latter. Near its origin the common carotid may give rise to the small inferior thyroid artery. It then passes to about the level of the larynx without giving off branches; here it gives off the superior thyroid (c) on the ventral side and one or more muscular branches (e) on the dorsal side. One or two centimeters further craniad it gives off on the dorsal side the internal carotid (g) and the occipital artery (f). The main artery now takes the name external carotid (m).
Fig. 119.—Common Carotid Artery and Internal Jugular Vein.
a, common carotid artery; b, internal jugular vein; c, superior thyroid artery; d, cervicalis ascendens artery; e, large muscular branches; f, occipital artery; g, internal carotid; h, branch to larynx; i, lingual artery; j, external maxillary; k, superior labial; l, inferior labial; m, external carotid; n, internal maxillary; o, posterior auricular; p, superficial temporal. 1, M. sternohyoideus; 2, M. sternothyreoideus; 3, M. geniohyoideus; 4. M genioglossus; 5, M. constrictor pharyngis medius; 6, M. constrictor pharyngis inferior; 7, M. longus capitis; 8, M. digastricus; 9, M. masseter; 10, M. scalenus; 11, M. levator scapulæ (cut); 12, M. levator scapulæ ventralis (cut); 13, M. splenius; 14, trachea.
Branches of the common carotid:
1. A. thyreoidea ima.—The inferior thyroid is a small artery which arises either from the common carotid near its origin, or from the innominate before the origin of the carotid. It passes craniad on the trachea as far as the thyroid gland, giving branches to the trachea and œsophagus.
2. A. thyreoidea superior (c).—The superior thyroid leaves the carotid opposite the thyroid cartilage and passes mediad and caudad, sending branches to the thyroid gland, and the sternothyroid (2) and sternohyoid (1) muscles. A small branch, the superior laryngeal, passes to the larynx, and supplies those muscles of the larynx which are not enclosed by the cartilages.
3. Rami musculares (e).—One or two branches, usually of considerable size, leave the common carotid at about the same level as the superior thyroid and pass to the muscles on the dorsal side of the neck, the main trunk of the artery passing between the longus capitis (7) and scalenus muscles (10).
4. A. occipitalis (f).—The occipital artery arises from the common carotid at about the same point as the internal carotid. It immediately sends a large branch dorsad, passing between M. longus capitis (7) and the vertebral column, to the deep muscles of the neck. The occipital then crosses the outer surface of the digastric muscle (8) to the back of the skull, and runs along the lambdoidal crest just beneath the splenius muscle. It sends a number of branches to the muscles of the back of the neck; and one of its branches may unite with the vertebral artery as it lies in the groove on the atlas, or with a branch of the vertebral.
5. A. carotis interna (g).—The internal carotid artery is one of the terminal branches of the common carotid. It is very small. It is given off near or in common with the occipital artery, passes toward the cranial end of the tympanic bulla, enters the bulla with the Eustachian tube, and passes into the skull at the foramen lacerum. Its course is much convoluted before entering the foramen. Within the skull (Fig. 121, g) it joins the posterior cerebral artery (Fig. 121, f) at the side of the hypophysis.
6. A. carotis externa (Fig. 119, m).—After giving off the internal carotid the continuation of the common carotid artery receives the name external carotid (m). It passes craniad and laterad between the digastric (8) and styloglossus muscles, where it gives off cranioventrad the lingual artery (i) and a number of small muscular branches; also sometimes the small laryngeal artery. At the dorsolateral border of the digastric (8) it gives off the external maxillary artery (j), and about one centimeter farther craniad the posterior auricular (o). It now turns mediad, lying against the cartilaginous auditory meatus, on its cranial side, and gives off the superficial temporal (p). The artery then continues mediad, taking the name internal maxillary (n)—so that the internal maxillary artery is to be considered the terminal branch of the external carotid.
Branches of the external carotid artery (Fig. 119):
a. A. lingualis (Fig. 119, i; Fig. 120, d).—The lingual artery leaves the external carotid near its beginning and passes craniomediad along the ventral border of the digastric muscle (Fig. 120, 9), accompanied by the hypoglossal nerve. It gives off numerous small branches to the hyoid and pharyngeal muscles, then passes dorsad of the hyoglossus muscle (Fig. 120, 6), where it gives off a branch which passes transversely across the middle line to communicate with the artery of the other side. Beneath the hyoglossus the artery turns craniad and passes into the tongue. Here it runs along the medial border of the styloglossus to the tip of the tongue, giving off numerous branches into the substance of this organ.
b. Rami musculares.—Muscular branches pass to the digastric and to the hyoid muscles. A small branch (Fig. 119, h), which may arise either from the external carotid or from the common carotid near the beginning of the external carotid, passes to the larynx and supplies the thyroarytenoid and lateral cricoarytenoid muscles of the larynx.
c. A. maxillaris externa (Fig. 119, j).—The external maxillary artery leaves the external carotid (m) opposite the angle of the jaw and at about the dorsal border of the digastric muscle (8). It passes craniad, lying at first beneath the digastric muscle and sending a branch to the submaxillary gland. Opposite the caudal border of the mylohyoid muscle it gives off the submental artery, turns dorsad, emerges from beneath the digastric, and passes along the cranial border of the masseter onto the face. Here it divides into superior (k) and inferior (l) labial branches, which pass along the upper and lower lips, respectively, giving off numerous branches.
The submental artery passes to the symphysis menti between the digastric and mylohyoid muscles, giving off on its course collateral branches to the muscles of this region.
d. A. auricularis posterior (Fig. 119, o).—The posterior auricular leaves the external carotid (m) opposite the middle of the bulla tympani and beneath the submaxillary gland. It passes about the base of the ear on its caudal and dorsal sides outside of the deep muscles of the occipital region, but beneath the auricular muscles, and sends several branches to the muscles of the external ear, passing onto the caudal surface of the concha. It sends also a large branch mediad to the muscles of the occiput, especially to the temporal muscle, within which it ramifies. A large branch (anterior auricular, Fig. 131, u) passes from the caudal side of the concha craniodorsad, and appears on the cranial side of the external ear, running along the cranial margin of the auditory opening.
e. A. temporalis superficialis (Fig. 119, p; Fig. 120, h).—The superficial temporal artery arises from the external carotid as the latter lies between the cartilaginous auditory meatus and the caudal border of the masseter muscle. It passes dorsad and gives off soon after its origin a muscular branch to the masseter, and an auricular branch which passes distad along the concha auris and ramifies over its cranial surface. The superficial temporal itself passes onto the surface of the temporal muscle (Fig. 120, 11), to which it gives numerous branches. It extends to the caudal angle of the eye (Fig. 131, s), where it divides. One branch passes into the lower eyelid; the larger branch passes along the dorsal side of the eye, sending a branch into the orbit and small branches onto the dorsal surface of the nose.
f. A. maxillaris interna (Fig. 119, n; Fig. 120, i).—The internal maxillary artery is the continuation of the external carotid. It turns caudad at the caudal end of the mandible, then passes craniad, lying dorsad of the pterygoid muscles (Fig. 120, 10), and against the medial surface of the mandible. It gives off the inferior alveolar artery (Fig. 120, j), then the middle meningeal (k), and then continuing mediad divides into three or four branches. The branches redivide, and the twigs form a complicated plexus, the carotid plexus (Fig. 120, l), which surrounds the maxillary division of the fifth nerve near its exit from the foramen rotundum. One of the larger branches of the plexus enters the skull through the orbital fissure, lying beside the hypophysis; it divides in the manner described below.
Fig. 120.—Branches of External Carotid Artery.
a, common carotid; b, branch to larynx; c, internal carotid; d, lingual; e, external carotid; f, posterior auricular; g, external maxillary; h, superficial temporal; i, internal maxillary; j, inferior alveolar; k, middle meningeal; l, carotid plexus; m, branch to temporal muscle; n, ophthalmic; o, infraorbital; p, lesser palatine. 1, M. constrictor pharyngis inferior; 2, M. sternothyreoideus; 3, M. sternohyoideus; 4, M. thyreohyoideus; 5, M. constrictor pharyngis medius; 6, M. hyoglossus; 7, M. geniohyoideus; 8, M. genioglossus; 9, M. digastricus; 10, Mm. pterygoidei externus and internus (cut); 11, M. temporalis (cut).
Beyond the carotid plexus a main trunk which may be considered the continuation of the internal maxillary passes craniad, lying on the dorsal surface of the external pterygoid muscle; nearly opposite the molar tooth it divides into the infraorbital (Fig. 120, o) and the sphenopalatine arteries.
Branches of the internal maxillary artery and of the carotid plexus:
1. A. alveolaris inferior (Fig. 120, j).—The inferior alveolar (or inferior dental) artery leaves the inferior maxillary just opposite the condyloid process of the mandible. It enters the mandibular canal by the mandibular foramen, along with the nerve of the same name, and traverses the canal, furnishing branches to the lower teeth. It emerges at the mental foramen, and its terminal branches are distributed to the chin, but a branch is continued in the bone beyond the mental foramen and supplies the incisor and canine teeth of the lower jaw.
2. A. meningea media (Fig. 120, k).—The middle meningeal is a large vessel which leaves the internal maxillary at about the same level as the inferior alveolar. It passes into the foramen ovale and ramifies in the dura mater. Its branches leave distinct impressions on the inner surface of the bones of the skull.
3. A large branch (Fig. 121, h) from the plexus passes into the cranial cavity through the orbital fissure and lies within the skull at the side of the hypophysis. It gives off the following branches:
a. A posterior communicating branch, very short, which extends caudad and joins the internal carotid artery (Fig. 121, g).
b. A. cerebri media (Fig. 121, i).—The middle cerebral artery passes dorsad on the side of the cerebral hemisphere along the fissure of Sylvius and divides into numerous branches which are distributed to the surface of the cerebrum.
c. A. cerebri anterior (Fig. 121, j) Passes dorsad between the cerebral hemispheres. Just craniad of the optic chiasma the two anterior cerebral arteries are united by a small communicating branch, thus completing the circulus arteriosus or circle of Willis (Fig. 121), surrounding the hypophysis (see page 292).
4. From the carotid plexus several branches pass, arising either separately or in common, to the masseter, temporal, and pterygoid muscles.
5. A. ophthalmica (Fig. 120, n).—The ophthalmic artery passes from the carotid plexus to the structures in the orbit. It gives off numerous branches which supply the muscles of the eyeball, and other structures of this region. It sends an ethmoidal branch into the nasal cavity through the ethmoidal foramen in the orbital plate of the frontal bone, then continues distad to emerge from the orbit on the medial side of the eye; here it anastomoses with branches of the superficial temporal.
6. A. palatina minor (Fig. 120, p).—The lesser palatine artery leaves the internal maxillary distad of the carotid plexus, near the caudal border of the maxillary bone. It passes ventrocaudad into the soft palate.
7. A. sphenopalatina.—The sphenopalatine is one of the terminal branches of the internal maxillary; it passes mediad through the sphenopalatine foramen into the nasal cavity, and divides into numerous branches which supply the mucous membrane of the nose. It gives off just before it enters the sphenopalatine foramen the descending palatine (A. palatina descendens), which passes into the posterior palatine canal and emerges on the surface of the hard palate, where it ramifies.
8. A. infraorbitalis (Fig. 120, o).—The infraorbital artery is a direct continuation craniad of the internal maxillary. It sends off numerous small branches to the teeth of the upper jaw, and a rather large branch which passes to the lower eyelid. It then enters the infraorbital foramen, at the same time dividing usually into two or three branches; these emerge from the foramen and supply the parts of the nose and upper lip adjacent to the foramen (Fig. 131, r).
A. subclavia. The Subclavian Artery.
The left subclavian (Fig. 118, c) arises from the convexity of the aortic arch just distad of the origin of the innominate artery, and about two or three centimeters from the heart. It passes craniad and slightly to the left, and turns into the left arm just craniad of the first rib.
The right subclavian (Fig. 115, n) is a direct continuation of the innominate, the artery receiving the name subclavian after the right common carotid is given off, usually at about the level of the second or third intercostal space.
The subclavian has the following branches: the vertebral artery (Fig. 118, g′), the internal mammary (Fig. 118, h), the costocervical axis (Fig. 118, g), the thyrocervical axis (Fig. 118, j). Beyond the last-named branch it continues into the arm as the axillary artery (Fig. 118, i; Fig. 122, g).