Fig. 11.—Railway servant’s cottage in the Roman Campagna, protected against the entry of mosquitoes by Professor Celli’s method.
The main obstacle to the adoption of the plan is undoubtedly the expense, which would amount to £20 or £30 for an ordinary Indian bungalow, and though this may appear by no means prohibitory in the case of permanent residents, it puts the matter practically out of the reach of even well-paid officials, as they can never count on enjoying the benefits of any permanent improvement of this sort for more than a few months; the wisdom of our rulers almost always leading them to transfer an officer to another station long before he is likely to have thoroughly learned his way about the streets of the town he has to govern.
Fig. 12.—Ground-plan of an existing up-country Indian Bungalow, to show method of adapting one (Professor Celli’s plan) of wire gauze protection. The dotted lines represent the wire gauze screens. D.G.D., double spring doors of wire gauze; S.G.D. single spring door of wire gauze combined with existing ordinary door; B.R., bath-room; D.R. dressing-room. Scale, 18′ = 1″.
On the preceding page is given the ground plan of an actually existing “up-country” bungalow of a very usual type in which the spaces guarded by gauze are indicated with dotted lines. The original doors are shown as complete, and the windows as shaded gaps. As will be seen, the number of doors for actual traffic is reduced to three, not counting those of the bath-rooms, which, being but little used during the hours of mosquito activity, have been left with single spring doors only.
There are many situations, such as houses necessarily placed in the midst of canal irrigation—Government canal bungalows for example—in which no other method of protection is in any way practicable, and it is clearly the duty of Government to protect officers, such as irrigation and forest officials, whose duties lead them into specially dangerous places, in this way in all cases where official quarters are provided. There cannot be the least doubt, too, that the capital so spent would be found to be a highly remunerative investment, and that this would be equally the case if steps were taken to protect all barracks in this way instead of wasting the costly soldier by needless invaliding. In the case however, of civil and military officers, who have to rent their houses from landlords, who are generally needy natives, with neither inclination, nor means, to provide costly improvements, the utmost they can do is to provide themselves with a sufficiency of portable folding gauze screens to protect their sleeping chambers. In any given locality there is generally some approach to a standard size for doors and windows, so that by the exercise of a little ingenuity it ought to be possible to adapt a set of folding screens to any room, allowing them when too large to overlap the sides of the embrasure, and supplementing deficiencies with sacking or rough planking. In India, for example, door openings are usually about 7 ft. by 4 ft., and screens opening out to this size might be utilised in most houses. It is obvious that the set of frames provided for each room must include one filled with a small spring door. I believe that a number of screens capable of opening out to something larger than the dimensions of an average doorway would be less bulky than any possible portable mosquito-proof room—and at any rate a complete set for an ordinary family would weigh far less than an average piano, and would be far more conducive to health. It should be added that in this, and in all cases where single rooms are placed under protection, all doors, internal as well as external, must be protected, and as they would in no way prevent the use of a punkah, they would be an enormous improvement on the ordinary mosquito net, which, failing such appliances, is an absolute essential to health during the malarious season.
Where nothing more permanent is possible, recourse must be had to mosquito nets, which can with care be made to afford a fairly thorough protection during the most dangerous portion of the twenty-four hours. It is a mistake, however, to trust to tucking the net in beneath the mattress, as this is apt to become disarranged during the night, and it is further very undesirable that the net should touch any portion of the mattress at all, as if it does so, the net can be also touched by the sleeper, who thus readily exposes himself to being bitten through the net. The top of the frame of the net should, therefore, be made both longer and wider than the bed and should be long enough to reach easily to the floor, with which its edge should be kept in contact by means of a hem weighted with sand or small shot.
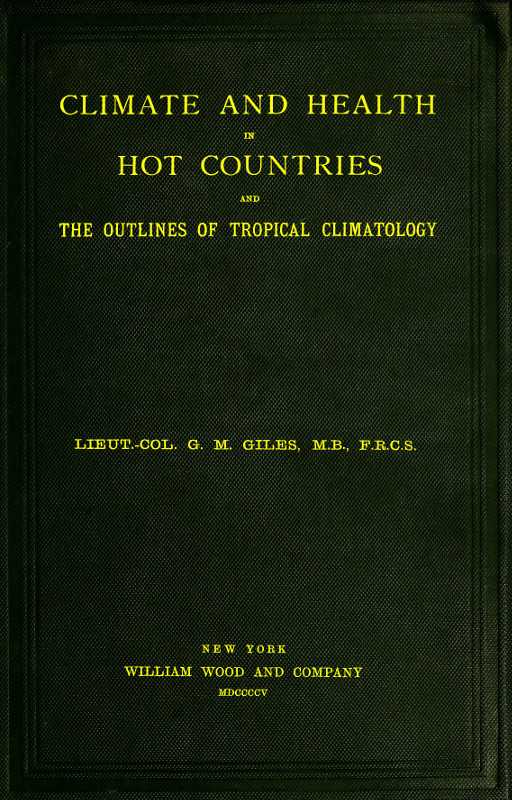
I have seen, especially in Calcutta, several attempts at the construction of curtains so large as to admit of a punkah being swung inside them, the top of the curtains being carried right up to the ceiling, and the strap of the punkah being pulled through a sort of sleeve; but the arrangement is necessarily an expensive one, and the swing of the punkah is always more or less crippled by the sleeve. A better plan is, I think, to make the frame supporting the netting very low, scarcely higher in fact than that of a child’s cot, so that the punkah swinging outside, but almost in contact with it, still passes within a foot or two of the sleeper. Such an arrangement is rather awkward to get in and out of, but this drawback is a very trifling one, compared with the enormous advantage of combining the protection of the net with the comforts of a punkah. For this idea I am indebted to Mr. Symmonds, of Rosa, whose contrivance I presume it is, as I have certainly never seen beds fitted in this way in anyone else’s house. For sleeping out of doors in the open, the net must, however, be of the usual fashion; as if the wind be at all strong, a weighted hem would not suffice to keep the net closed. It is therefore important when sleeping out to use a large bed, so that contact with the net may be less likely to happen; and the top of the net should be formed of ordinary calico, so as to keep off the dew. Not unfrequently the mesh of the netting sold for making mosquito nets is too coarse, a point of some importance, as Anopheles mosquitoes in particular are adepts in creeping through small openings; and as the writer has found it impossible to confine them in enclosures formed of the coarser patterns of net, it may be concluded that such a material is equally inadequate to keep them out.
Fig. 13.—Bed arranged with a low mosquito-net frame, with punkah above it.
References to the protection against malaria afforded by mosquito nets by observant sportsmen and explorers are to be found in numbers of books of travel and adventure published long before any explanation of the fact was possible; and during the malarious season it is nothing better than culpable rashness to pass the night without this protection, except in a room properly guarded with wire netting. It is quite common to hear it asserted that a punkah alone is sufficient protection, but this is an entire mistake, as I have repeatedly watched a mosquito making a comfortable feed on my person within a few inches of a spot actually flicked by the towel which it is usual to pin on to the lower edge of the punkah. In non-malarious months, such as the hot dry weather preceding the rains in northern India, there is, of course, no need of a net except as a matter of protection against the harmless, but very annoying, Culices that are very common at that season of the year; and in spite of its inferior protection against being bitten, many will prefer the freer air current afforded by the punkah. After the commencement of the rains, however, the fact cannot be too strongly emphasised that to sleep without the protection of a net is to wilfully expose oneself to a real and ever-present danger.
In the matter of preventing mosquitoes from becoming infected it is obvious that comparatively little can be effected by the private individual. All he can do is to bear in mind that persons suffering from malaria are as great and real a danger to their neighbours as those affected with scarlet fever, small-pox or any other communicable malady, and accordingly to try to limit the number of such cases amongst his servants and dependents. In the great majority of cases in all probability, the mosquito that infects the European resident has been infected by a case amongst his servants; and quite apart from philanthropic considerations, it is most important to detect all such cases and have them treated with quinine.
It is a well-known fact that, even where the drug appears to fail to cure the disease, it is very difficult to find the malarial parasite in the blood of cases that have been well dosed with the drug, and as there must be parasites present in the blood itself in order to convey infection to the mosquito, it is obvious that, apart from its curative action, quinine may also be said to act as a disinfectant. On this account, where the removal of a servant “down with fever” cannot be arranged, it is highly important that he should be liberally dosed with quinine; and it must be remembered that it is not sufficient to supply him with the drug, but that it is also necessary to see it taken. In some countries, the native is so truly a child in intellect, that he has to be treated like one if a bitter drug is to be administered; while the Indian, though in no way wanting in intelligence, has often a prejudice against quinine owing to the active propaganda against the drug preached by the Baids and Haqims, or practitioners of the indigenous systems of medicine. As a matter of fact, I believe these men use quinine largely, but they take care not to let their patients know they are taking a drug which can be got for a halfpenny a full dose at any post office, and try to prevent the spoiling of their market by promulgating all sorts of fables as to its dangerous and harmful character.
According to the queer phraseology in vogue amongst these folks—and it is not so long ago since it was employed also in Europe—fever is a cold disease which by an attractive paradox should be treated by cold remedy, while quinine is made to belong to the opposite category of medicinal agents. It is as well, then, to be prepared for objections of this sort; but, as a rule, the personal influence of an European employer will suffice to secure the taking of the medicine, provided he will take the trouble to personally see it swallowed.
Liable as all residents in the Tropics are to be attacked with fever at times and places where skilled medical assistance is not obtainable, it may be well to conclude this chapter with a few words on the treatment of the malady. This really resolves itself into the adequate administration of quinine; for provided a sufficiency of the drug can be got into the circulation, it will, I believe, always cure malaria; but it is one thing to make the sick man swallow the drug and another to secure a sufficiency of it being absorbed into the blood; and unless this takes place, the remedy can have no more effect than as much oatmeal or any other inert substance. Anyone who has suffered from a severe attack of malaria, or had the nursing of a case, must have noticed that want of power to tolerate or digest even the lightest food, is one of its most prominent symptoms. In the more virulent type of the disease, nausea and vomiting is one of its most distressing features, and are nothing more than the outward manifestations of the fact that the digestive organs have ceased to perform their functions, and this may be equally the case, even where these additional evidences of the fact are not so prominent.
A little reflection will show that it is very unlikely that quinine or any other drug will be absorbed by a stomach that can no longer deal with even the lightest food, and hence it is not surprising that the severer forms of remittent fever will often resist quinine for long periods. For the same reason that quinine so often fails to do good in virulent cases, it is equally obvious that it is unlikely to do harm, and the absurd theory that “blackwater fever” is the outcome of treating malaria with quinine may now, I think, be said to be abandoned by all, save perhaps one or two of its original propounders; for though quinine appears to be of but little value in the treatment of that doubtfully malarial disease, it has now again and again been shown to occur in patients who have taken no quinine at all.
It cannot, therefore, be too strongly insisted upon that, in spite of failure to produce immediate effects, the administration of quinine should be steadily persisted in, as sooner or later in almost all cases a sufficiency will be absorbed to check the disease.
From what has been said, it is clearly important to do our best to put the digestive organs, if possible, in a position to perform their functions, and as in the majority of cases the sluggish bowels are loaded with half-digested or undigested food, it is a good general rule, as a preliminary to the administration of quinine, to administer some unirritating laxative, for which purpose nothing can be better than our old friend and bugbear of childhood, castor oil; and the dose should be repeated whenever constipation becomes a symptom in the course of the case. Once the laxative has acted, the sooner quinine is administered the better, and, unless the patient be one of those unfortunately constituted persons who are unable to take it—and there are some few to whom quinine seems as poisonous as it is to the malarial parasite—it should be given in full doses to the extent of 20 or even 30 grains (1 to 2 grammes of metric system) in the twenty-four hours. A dose of 10 grains, followed by others of 5 grains each, will usually be found a convenient plan of administration; but there are cases which do better with smaller doses more frequently administered. The best way to give it is, I think, to stir up the powder in a little milk; and it may be well here to offer a word of caution as to the employment of the drug in the form of tabuloids. For some reason, the drug appears difficult of digestion in this form, for I have repeatedly found fever yield at once to the ordinary powdered form of the drug, after days of fruitless treatment with quinine tabuloids obtained from firms of so high a reputation that the suggestion of the substitution of some less expensive material for quinine is quite untenable. The indiscriminate use, too, of antipyrin, phenacetin, &c., is also to be deprecated. They are all powerful depressants; and though they afford great relief to the aches and weariness of an attack of fever, undoubtedly have no effect whatever in curing the disease, even if they do not, as I have often been inclined to suspect, tend to prolong it. Where the suffering is very acute, an occasional dose may be of use for securing rest, but anything like continuous dosing with medicines of this sort should be carefully avoided. On the other hand, the old-fashioned “fever mixture,” composed of ten or fifteen drops of nitrous ether with a drachm of Minderus’ spirits (liquor ammoniæ acetatis), every four hours, in a wineglass of water, is often of great use in favouring perspiration, besides acting as a useful diuretic; and may be recommended as not only affording much relief to the patient’s subjective symptoms, but also of being absolutely safe even in inexperienced hands.
Except in the weakness of very prolonged attacks, stimulants should be but sparingly given, but they should not be withheld when the patient is flagging, and obviously falling into what is known as a “typhoid state.”
It is almost needless to remark that care is required in the matter of diet. During the febrile periods “slops” only should be given, and then in not too large quantities at a time; but in those cases where there is a distinct fever-free interval between the paroxysms of the disease, a great deal of license may be allowed, and solid food of a light digestible sort is often not only well tolerated, but even beneficial, while it is almost needless to say that these intervals of returned digestive power should always be seized upon to get a liberal supply of quinine into the system. During convalescence the administration of 10 to 15 grs. a day of quinine should be maintained for at least a week after the disappearance of all febrile symptoms, and some ordinary tonic, such as Easton’s syrup, is often useful in facilitating the return to strength.
The least sign of a relapse, as evidenced by a rise of temperature, of however temporary a character, should be met with a further treatment with quinine for at least a week or ten days, as it is a clear sign that the disease is scotched, but not killed, and that some of the parasites are still lingering, in a latent condition, within the system; for the patient cannot really be considered as cured till the last of these is put an end to.
The length to which this chapter has attained may be justified by the fact that the universality and the extent of the mischief wrought by malaria in tropical climates renders the subject by far the most important of all in connection with the preservation of health in the tropics; and the writer trusts his readers may be moved to do as much as they possibly may to preserve themselves and their neighbours from the havoc wrought by this insidious disease, for without an informed and intelligent public opinion to back them, no possible efforts on the part of sanitary officials and medical men can be expected to exercise any great or lasting effects on the prevalence of the disease.
CHAPTER VIII.
On the Prevention and Treatment of Certain of the more
Common Tropical Diseases.
Although the main essentials of domestic sanitation have already been dealt with at some length, and incidental mention has necessarily been made of their bearing on the avoidance of particular maladies, it appears desirable to devote a few pages to the separate consideration of the avoidance of some of the more common tropical diseases. Some apology may be necessary for the inclusion in the following remarks of some brief references to medical treatment, but it is difficult to keep absolutely distinct the subject of prevention and cure in a popular work, and while there is no desire to convert this little book into a treatise on family medicine, it is thought that a few words on the subject of remedial treatment may not be out of place, especially as most of the writers that treat of this subject popularly, from the tropical point of view, are hopelessly out of date.
It must be clearly understood that what little is said on this subject is in no way intended to supersede the necessity of medical advice, whenever that may be available; but in these out-lands, the number of doctors to the square yard is far smaller than it is in Europe, and even in comparatively settled regions, it is quite easy to place twenty miles or more between yourself and the nearest medical man.
It must be remembered that in tendering general advice of this sort the prescriber is considerably hampered by the necessity of recommending nothing that is likely to do harm should the amateur doctor’s diagnosis be faulty, and that he is thus debarred from suggesting many measures that would be perfectly appropriate were the case under competent supervision.
I do not of course refer merely to the question of poisons, as there are few drugs that are of any real use that are not capable of causing dangerous symptoms if administered in adequate doses—and many of the drugs recommended are as a matter of fact powerful poisons—but rather to the fact that even assuming reasonable care and intelligence in weighing and measuring, one must needs direct only such measures as will not be harmful in the by no means unlikely event of a mistaken diagnosis. In only too many of the scourges that devastate these latitudes, there is no time to wait for the arrival of a doctor living a day’s journey away, as the chances are that the fate of the patient will be no longer in the balance when at last he arrives; so that for anything to be of any use it must be done quickly.
This method of treating the subject necessarily involves occasional repetition, but in view of the importance of the details thus emphasised, this may not be entirely disadvantageous.
Cholera.
When the writer first went to India some quarter of a century ago, there was still a tendency to invest this disease and its propagation with certain mysterious attributes, and a certain pompous obscurantist who was then at the head of affairs invented the awe-inspiring term of “pandemic waves” to account for, or rather cover, ignorance as to its method of spread; nor was it altogether safe for his subordinates to record facts that appeared to indicate a more common-sense explanation. But even then, the theory that the disease was usually conveyed from man to man by infected water, was held practically by all whose opinions were worth having. Still we were very much in the dark as to the methods whereby it gained access to water, and had no means of distinguishing infected from harmless water; and our measures of prevention, being thus based on guess work, were uncertain and often ineffective. At the present day, thanks in the main to the labours of Koch and Hankin, there is no disease about which our knowledge is more definite. In dealing with semicivilised communities it is still, it is true, quite impossible to prevent or foresee outbreaks of the disease, but when it occurs our knowledge now enables us to bring an epidemic to a speedy termination, always provided we are permitted to do so by the population; and personal prophylaxis may almost be said to amount to security.
We now know that the germs of cholera can exist only in the human organisation, but that they are capable of living and also multiplying in water. In very impure water, they cannot long survive, as they soon get crowded out of existence, in such situations, by putrefactive and other germs that are most at home under such conditions. For their multiplication the presence of a certain amount of otherwise harmless organic and mineral matter is of course necessary, but if introduced into water containing this, they can survive some time in the purest natural waters, though they ultimately die out in such situations. Owing to these habits of life on the part of the germ, it follows that the taste and appearance of water are absolutely valueless as regards its safety, and that the chemical examination of water is an equally futile test. The disease is carried about from place to place by infected human beings; but in ninety-nine cases out of a hundred is conveyed from man to man not directly, but indirectly through the agency of drinking water. In the hundredth case the germs may be carried in food, and of course milk, being often intentionally or accidentally mixed with water, is a frequent vehicle.
Direct infection from man to man does probably occasionally occur, but the contingency is too remote an one to be worthy of consideration, as it implies close personal contact, and in fact is usually traceable to those in attendance on the sick getting their hands or clothing fouled with the discharges and neglecting due measures of disinfection before eating or drinking. Save in this way, there is practically no risk whatever in the proximity of, or of attendance on, cholera cases, and no one need shrink from nursing persons stricken down with the disease, provided they observe a few very obvious precautions.
Fortunately the cholera germ is rather a delicate sort of plant, and but for its sharing with man a preference for good drinking water it would be comparatively harmless, as it soon perishes elsewhere, and is very soon destroyed by drying or too great heat. It is needless to remark that it cannot stand boiling, for the germs that can stand that sort of treatment are few and far between; but it is also very sensitive to the action of most of the ordinary disinfectants, which destroy it in dilutions far weaker than is the case with the agents of most other diseases; and it is also killed by a sufficiently long exposure to the action of carbonic acid, from which fact there outcomes the useful bit of knowledge that it is quite safe, qua cholera, to drink aerated waters even of doubtfully careful preparation, provided that they have been kept a few days in the house before use. Owing to the fact that the cholera germ cannot only survive, but is also capable of multiplying, in drinking water of average purity, the amount of fouling of the water which is required to infect it may be very small indeed, and usually is infinitesimally small.
A traveller draws water from an infected, but chemically practically pure well, and marches on, or it may be travels some hundred miles by train. Arrived at his next halting-place, he lowers his drinking vessel into the well he finds there. The amount of matter carried from the infected to the clean well is necessarily far too small to turn the most delicate balance ever constructed, but that same amount would suffice to infect not one, but an indefinite number of wells, so infinitely small are the individual germs concerned carrying the infection. Moreover, the drinking of infected water does not imply certain infection, as at certain stages of digestion the germs are destroyed in the stomachs of healthy people; and hence it is quite possible for the disease to be introduced by a person who has not himself suffered, though perhaps it is more common for it to be caused by mild cases; for it is a mistake to think that cholera is always a fatal or terribly serious disease, as in every epidemic large numbers of cases occur of slight upset of the digestive organs, but which we now know by microscopic examination to be really true cholera. These cases, however, are rarely recognised or recorded, and the really virulent form of the disease, which kills, roughly speaking, half of those it attacks, is alone referred to in ordinary statistics of attacks and deaths.
In India, and I suspect in most other semicivilised countries, the commonest method by which wells become infected is by the using of a vessel which has contained infected water to draw water from an uninfected well. The quantity of material required to start the fermentation in a still wholesome well is, as already remarked, infinitesimally minute, and a small drinking vessel and the string used for lowering it into the water, if carried by a traveller from an infected to a healthy place, is amply sufficient, and as the, chemically speaking, still pure water of an infected well is all that is required, it is obvious that no actual fouling of drinking water with the discharges from those stricken down by the disease is either necessary or common. The actual fouling of wells from contiguous latrines or cesspits does no doubt occasionally occur, but owing to the extremely primitive character of Oriental plans of conservancy, is rare.
From what has been said, it will be obvious that it is perfectly easy to suggest measures for the prevention of cholera which may be trusted to be perfectly effectual. The only difficulty lies in carrying them into practice. Practically, all that is required is to protect all supplies of drinking water by covering in wells and fitting them with pumps. But the mere expense of doing so is often beyond the means of the community, and when the pumps have been fitted, there is no one available to keep them in order; so that after a very short period they become useless, and the old infection-carrying bucket and string must needs be reverted to. Nor is it by any means easy to protect one’s own supply, as strangers have a free and easy way of making use of their neighbours’ wells, whether rich or poor. Nor can one’s native servants be trusted either to prevent this or to employ for drawing water a single vessel set apart for the purpose, for being unable to comprehend the reasons for such precautions, they naturally regard them as merely troublesome fads on the part of their employer, to be observed only when he chances to be looking on.
On this account the cardinal precaution of personal hygiene is to drink only water that has been boiled, and to see it boiled oneself. Every housewife knows that even European servants are often singularly obtuse, or neglectful, in recognising when water has actually come to the boil; and that to be certain of the perfection of the domestic cup of tea she must satisfy herself that the water is actually in a state of ebulition. Nor are such precautions onerous or troublesome. Orders should be given that the portable charcoal stove should be brought into the verandah and that the water should be boiling at the time of some meal, when the master of the house necessarily passes through on his way to table; preferably that of late dinner, so that the water may have all night to cool in, and so be ready for the next day’s consumption. The boiling water should be poured directly into the vessels, porous or otherwise, in which it is to stand, and put aside in some place sheltered from dust. They should not be filled too full, as after they have cooled it is desirable to shake the water violently so as to re-aerate it, and so remove the insipid taste which the water has acquired, owing to its dissolved air having been expelled during the boiling process. The still boiling water may generally be trusted to sufficiently sterilise the containers, but it is perhaps well, as an additional precaution, to boil them occasionally in a large cauldron. Above all, do not filter; but trust to settlement. Ordinary filters are perfect germ-traps, while all varieties of the Pasteur filter are slow in action and apt to get out of order. Added to this, their rubber connections may leak without our being aware of it, and even when in their most perfect condition, they afford a protection but little superior to that given by boiling, so that personally I would far prefer to put up even with a little turbidity in boiled water than put any trust even in the best of them. Remember that you can trust no one but oneself to attend to their cleanliness and efficiency, and that to do so implies the sacrifice of a good deal of time on a very irksome job. Drinking water that chances to be impregnated with lime necessarily becomes turbid on boiling, but the turbidity is perfectly harmless. If the deposit be so fine as to be very slow in settling, the process may be hastened by stirring it round a few times with a crystal of alum. These precautions should be, of course, routine ones at all times, but should be maintained with special vigilance at times when cholera is present in one’s place of residence. Aerated waters that have been kept in the house a week may also be drunk, but care should be taken to avoid any articles of food that are consumed raw, such as salads and fruits. Tomatoes may be dipped into boiling water and peeled without detracting from the pleasant, fresh acidity of their taste, but it is well to specially avoid during such periods lettuces and melons, as owing to the circumstances under which they are cultivated they are specially liable to have been wetted with infected water. Cucumbers may be dealt with in the same way as tomatoes, as from their shape it is very easy to sterilise their exterior by dipping them for a few seconds beyond the middle of their length in boiling water and changing end for end. This and the customary subsequent peeling really affords a sufficient practical security, and it must be remembered that the usual dressing of vinegar, “fortified” as this article of consumption usually is with sulphuric acid, affords an additional security, and does away with the necessity of submitting to what would be really a considerable deprivation at the time of the year when cholera is most common; for cholera and cucumbers flourish most at the same season of the year, a coincidence which has led to the not unnatural, but quite erroneous, popular idea that cholera may be caused by eating this vegetable. Of course, too liberal an indulgence in cucumber, like too much of any other rather indigestible good thing, may cause bowel disturbance, and an irritated bowel is especially liable to infection; but apart from superadded infection, no article of food is capable of causing the disease.
In dealing with drinking water on a large scale, such as the disinfection of wells and tanks, we have several available methods, for one or the other of which the materials are almost everywhere available. The most valuable of these agents is undoubtedly the permanganate of potash, and the suggestion of its use for the disinfection of drinking water from the germs of cholera is undoubtedly due to Mr. Hankin, our official bacteriologist at Agra. No doubt more than one medical officer had previously made experiments with this chemical for the purification of drinking water, but the credit of definitely proposing its use on a large scale in cholera epidemics, and of proving that it is lethal to the cholera germ, even when greatly diluted, is undoubtedly due to him alone.
The enormous practical importance of the discovery has, however, been but slowly realised, though its capabilities were put to the test of practical application by the writer immediately after Mr. Hankin published his suggestion, with the result that a severe epidemic in a town of over 10,000 inhabitants was brought to an abrupt termination within three or four days.
The method of disinfection of wells by means of this chemical has already been described on page 47, et seq.
The addition of a few ounces of common sulphuric acid increases, I believe, the lethal effects of the permanganate on the cholera germ, but is certainly not necessary, and I have no personal experience in its employment, as the taste imparted is somewhat persistent; and in dealing with suspicious races such as those inhabiting our Indian possessions, it is desirable that all obvious change in the taste or appearance of the water should pass off as soon as possible.
The alternative agents are alum and quicklime, either of which is very fairly effectual, though by no means as trustworthy as permanganate. Their great advantage lies in the fact that they are obtainable almost everywhere, and that being familiar articles of daily life their use is less likely to give rise to misunderstandings in dealing with ignorant and suspicious populations, who regard with mistrust the treatment to their wells with a chemical so strange and striking as permanganate must appear to them. Nearly all races are, however, familiar with the cleansing powers of lime, and in the case of Indians, the wonderful powers of alum in clearing turbid water is a bit of household knowledge familiar to everyone. A pound or two of alum, or half a hundredweight of lime, are required for each well. If alum is employed, it should be roughly powdered.
To further avert all suspicion I find it a good plan to hand the necessary money to an inhabitant of the place and ask him to fetch me from the local shop the amount of alum or lime required. I then, if alum be chosen, tell him to pound it up with a brick and himself to throw it into the well, myself standing somewhat aloof. As everyone is familiar with the use of alum in purifying water, and there is obviously no possibility of the surreptitious introduction of anything else, with ordinary tact, no objection will ever be made. Of course, the person thus impressed into the service of sanitation should always be a man of good caste, preferably a Bhraman.
Both these agents act, I believe, mechanically by coagulating certain forms of organic matter present in the water, and so carrying to the bottom, entangled with it, the germs present in the water, in which situation they perish on account of the free access of water containing their nourishment being impeded, and on this account at least two days should be allowed to elapse before the water is again taken into use, during which all disturbance of the water should be carefully avoided.
Neither of these agents is in any degree as trustworthy as permanganate, but their employment should not be neglected in cases where the latter is either unobtainable or objections are raised to its use. Of the two, lime is probably the better, but alum much the handier.
Whichever agent be adopted, it is well to treat as large a number of wells as possible. A certain number must needs, of course, be left untouched, for use during the time the treated wells must be left undisturbed, and these should be dotted about the town, so that the minimum of inconvenience may be inflicted on the townsfolk; but always leave as few as possible, as objections may be raised on your second visit, a couple of days after, to complete the process by disinfecting the remaining wells, and it may hence happen that you may have to rest content with what you have been able to effect on your first visit. Always, too, commence operations on the well you have reason to suspect is infected, or, in other words, that used by the people of the house in which the first local case has occurred.
Permanganate has now had a long trial in India. I have never known it fail, wherever it has been used in the manner above described, and the operation has been conducted by an European officer in person. The native medical officer, even when trained after our European methods, is seldom really convinced of its efficiency, and moreover he lacks the prestige of prophets hailing from abroad, and so may be really unable to carry out his instructions. An even commoner mistake is to go to work piecemeal, disinfecting a few suspected wells and leaving the rest till fresh cases spring up, as they necessarily must, as buckets infected from the first infected wells will inevitably be taken to other wells during the time that the former are unusable, and they can scarcely fail to infect them, and so start new foci of infection, if sufficient time be allowed for the germs to increase and multiply to a dangerous extent in their new location. Reports of failure I have received in plenty, but on investigation they have always proved to be due to some such cause as those indicated above. It is, of course, only rarely that a layman will find himself called upon to conduct such operations on a large scale; but the knowledge of how to do so may be of such great public benefit to the readers’ coloured fellow-subjects, that it is most desirable that every European should know how to proceed, and, at any rate, I would strongly advise my readers, should cholera appear in their neighbourhood, never to omit the precaution of disinfecting all wells under their own control, as it is a great protection to one’s servants and other native attendants. It is well, too, to repeat the process occasionally as long as the disease continues near one.
By the simple precautions as to food and drink described above, the danger of being attacked by cholera may be reduced to a very small contingency, even when it is raging around one, and there is no reason whatever for the almost superstitious fear with which the disease used to be regarded.
It remains to say a few words as to the treatment of cases should they arise in your household in places where medical aid is unobtainable.
In the first place, it should be remembered that the danger of handling and nursing patients is but small, for, as already remarked, you cannot “catch” cholera in the same way as you can small-pox or plague. To become infected by the germs you must eat or drink them. The discharges in cholera are, of course, intensely poisonous, and it is impossible to nurse a case without the hands, and perhaps one’s clothing, becoming fouled; but the germs are perfectly harmless applied to the skin, and with due precautions as to cleanliness and disinfection of the hands, there should be no danger of their gaining access to the nurse’s mouth. To avoid contamination of clothing, a washable overall should be worn, such as can be improvised from a sheet, with a hole for the head cut in the middle, secured round the waist with a cord, and the sleeves should be turned up well above the elbows. Care should be taken not to touch the lips or face with the hands while in attendance on the patient. On leaving him, the overall should be wrung out in sublimate lotion and spread out in the full blaze of the sun to dry, and the hands and arms should be thoroughly washed first with warm soap and water and then with sublimate lotion, care being taken not to eat or drink until these precautions have been complied with.
Medical science is absolutely at fault in the treatment of cholera, so that no treatment can be recommended beyond such measures as naturally suggest themselves to relieve the patient’s sufferings.
The symptoms of the disease consist of violent purging and vomiting, the discharged matter being watery and almost colourless, with small particles and shreds of whitish matter floating in it, being, in fact, to quote the usual simile, very like rice water. Very often the patient suffers from violent muscular cramps, which cause great suffering. This active onset is followed by a stage of collapse, in which the skin becomes cold and livid and the face and hands singularly pinched and blue. If the patient survive this stage, it will be found that the urine is suppressed, the functions of the kidneys being, for the time, absolutely suspended; and the patient can never be considered out of danger till this function has resumed its natural course.
Now as to treatment. It must be in the first place remembered that it is absolutely useless to worry the patient with attempts to administer medicines by the mouth, as the digestive and absorptive functions are for the time totally stopped, and it is quite as much to the purpose to put your remedies in the patient’s pocket as to force him to swallow them. To have any chance of acting, medicines must be administered by being injected beneath the skin by means of the hypodermic needle; and so powerless are all known drugs in this disease, that I should hesitate to recommend such medications to be attempted by amateur physicians. The only drug which has ever appeared to me to effect any good has been chloral hydrate dissolved in water and injected under the skin in 5-grain doses every few minutes until 30 or even 40 grains have been administered. There can be no doubt that this treatment controls the violence of the symptoms, and usually does away with the horrible suffering caused by the terrible cramps that are so common in the disease. I am even inclined to believe that a somewhat better percentage of cases recover under the treatment, though this is doubtful. Failing this, massage and frictions with the hands do much to relieve the cramps, and in the cold stage, every care should be taken to maintain the heat of the body by covering the patient with blankets and placing around him bricks heated in the fire and wrapped round with strips of wet blanket. During the reaction that follows on the cold stage, in favourable cases, attempts should be made to stimulate the kidneys by the application of mustard plasters to the loins. To attempt to give food during the acute stage is obviously worse than useless, but there is no harm in letting the patient suck small lumps of ice to assuage the terrible thirst of the disease. In the stage of collapse, stimulants naturally suggest themselves, but are seldom of any use when given internally. A few drops of ether inhaled from a handkerchief is, if available, perhaps the best method of stimulation, but the weakened kidneys have quite enough to do without having to deal with alcohol, so that it should be but sparingly resorted to, if at all. When the patient shows such signs of recovery that it appears likely that food can be tolerated, small quantities only of easily digestible food, such as milk, rendered mucilaginous by the addition of a little arrowroot, Brand’s extract, &c., should be given, but it can easily be understood that after so severe a shock to the digestive system, the greatest care will have to be exercised in the feeding of the patient. Finally, it should not be forgotten that all the discharges of the patient are virulently infective, and that they and everything soiled by them should at once be disinfected. When the supply of disinfectants is limited, a good plan is to place in the bed-pan and basins used a sufficiency of sawdust, and to at once burn the contents by emptying them on to a brisk fire.
Dysentery.
We cannot claim to know much definitely as to the exact method in which this disease arises. Four or five vegetable germs and at least two small parasites belonging to the animal kingdom have been found, but none of these are present in all cases, and many of them may be quite commonly discovered in the interior economy of quite healthy persons, so that either the true germ remains to be discovered, or those we know of have only a secondary importance, becoming harmful only when they find themselves in contact with an irritated bowel. As a matter of fact, there are a good many kinds of dysentery, but to enter into their various characteristics would only confuse the lay reader.
The common characteristic is the discharge of frequent scanty motions, with much pain, and an intolerable sensation that more is to come. The material voided is always extremely offensive, of a mucous consistence, and wanting in the natural bilious colour. In severer cases, the mucus becomes streaked with blood, and sometimes little else will be seen, and the actual loss of blood itself may become a serious element of danger.
The disease does not usually occur as an epidemic, though something very like one is not unfrequently to be met with among bodies of men subjected to severe hardships and privations, as for example among soldiers during an arduous campaign in extreme climates. Some predisposing cause capable of causing irritation of the intestine seems to be essential to enable the germs, known or unknown, to take action. This irritant may be mechanical, such as coarsely ground, ill-cleaned grain; or chemical, as in the dysentery that is apt to appear among persons feeding on too newly reaped barley, or from foul or saline water; but the commonest of all causes appears to be the decomposition of the contents of the bowel which almost inevitably occurs when, from any reason, the production of the bile is arrested.
The peculiar yellowish-green secretion of the liver known as the bile appears not only to assist in the solution and digestion of the food, but to act as a natural antiseptic, which checks the too great multiplication of the various germs which are naturally always to be found in the intestine. It is comparatively rarely that the liver itself strikes work, but what does very commonly happen is that a chill, or a mechanical or chemical irritation of the bowel, may extend to the bile duct, and by causing swelling, or spasmodic action of its muscles, prevent the contents of the gall bladder, in which the bile secreted by the liver is stored up, from passing on into the intestine. The chill or irritant that thus stops the flow of the bile necessarily at the same time produces a greater or less amount of catarrh and inflammation of the lower bowel, which, lying as it does next to the wall of the abdomen, is most easily affected by cold; but stoppage of the flow of bile into the intestine seems an essential element in the production of dysentery, as a more or less complete absence of bile from the motions is a universal symptom of the condition, and to restore the action of the liver is, practically speaking, in cases taken sufficiently early, equivalent to curing the disease.
As has been already noticed, dysentery may be caused by a variety of mechanical and chemical irritants, but by far the commonest cause is undoubtedly chill to the surface of the abdomen, and the reason the disease is so common in tropical climates is their peculiarly treacherous feature of the chill that precedes the dawn. The earlier part of the night is often intolerably close and sultry, and it is only with difficulty that the jaded European manages to get off to sleep, and then naturally with next to no covering of the body. As the hours pass, the temperature falls somewhat and he sleeps more easily and deeply, and when the peculiar chill falls that usually precedes a tropical dawn, he is too far off in the land of dreams to be roused by the cold; and the abdomen, bared probably by his restless movements during the earlier part of the night, is left exposed to the treacherous chill.
That there are other ways of getting dysentery I have no doubt, but a tolerably long experience has convinced me that the above is the history of nine cases out of every ten that one meets with, and it follows from this that the all-important safeguard against dysentery is to protect the abdomen from chill. From this it follows that a cardinal measure of precaution in the preservation of health in hot climates is the adequate clothing of this part of the body. It is this fact that accounts for the general consensus of opinion as to the value of the familiar article of clothing known as the “cholera belt,” though I am by no means inclined to regard the said garment as the best, or even a good, method of attaining the object. At best the thickness of material is inadequate, it is generally made too narrow to include the liver above and much of the lower part of the abdomen below within its protection, and it naturally has a strong tendency to “ruck” together so as to form merely a very uncomfortable sort of belt, quite valueless for the purpose for which it is intended. For wear during the day a much more comfortable and efficient garment is the well-known Oriental “kamarband,” a long, narrow scarf of woollen, cotton, or silk, according to taste, folded into a broad band and worn twisted round the waist in place of a waistcoat, over which it possesses the superiority of leaving the upper part of the body free. The elasticity of the folded scarf gives also a comfortable feeling of support, without any of the sensation of constriction inseparable from a belt, and its adaptation to climatic needs is testified by the fact of its being, in one form or another, in use by every tropical race, if we except the Negro, who seems to the manner born, and to want little artificial protection while he keeps within the limits, to meet the conditions of which he evolved. How the Negro gets on with no clothing at all, and the really much civilised Bengali contrives to survive without a hat, are problems which we poor products of centuries of artifice cannot be expected to solve; but the bald fact remains that the Northern European, when translated to the Tropics, must protect his viscera against cold in equatorial climates, even more carefully than in his native north, if he wants to get back there alive.
The cholera belt is especially fallacious at night. Unsupported as it then is by other clothing, it is at no other time so liable to slip down and leave unprotected the very parts that it is most important to keep covered. In the dark hours one wants a protection that is unlikely to be disturbed by forgetfulness, and is more likely to fall back into place than be cast off. This exigency is met by a folded blanket thrown across the trunk, within which are massed the delicate viscera essential to life; the ends of the folds lying on either side on the ground, and folded so that, without too thoroughly rousing oneself, one can spread the rug out a bit, above or below, should the chill of the morning become disagreeable to the chest or the lower limbs.
Provided that the feet, chest and arms are left free, a blanket arranged in this way gives no feeling of oppression; and after a short period of habituation, its deprivation conveys a distinct sensation of discomfort. Lying across the body, with either end on the ground, it is unlikely to be disturbed by the uneasy movements of the body. The fact of the ends resting on the ground makes it difficult to shake it off, and it affords far better protection than any closely-fitting garment, is more comfortable, and less likely to cause prickly heat. Care in this matter, especially during the hours of sleep, is second only in importance to the protection of the head against the sun during the day.
Never let the mildest dysentery, or even diarrhœa, continue unchecked. Taken early, no disease is more tractable, while if allowed to pass on to a chronic condition, no malady is more troublesome; while really severe chronic dysentery is practically incurable. Some knowledge of how to deal with such cases is therefore of special importance, as without embarking on the career of an explorer, any one may find himself a day or two’s distance from competent medical assistance in the countries with which we have to deal.
Practically speaking, to restart the action of the liver is to cure dysentery in all recent cases, and hence it is of the greatest importance not to give opium, or that dangerous abomination “chlorodyne,” both of which are most efficient in diminishing the flow of bile. They are doubly dangerous, because they quiet not only the action of the gall bladder, but also that of the intestines, and this, it must be remembered, without really curing the disease. The flux from the bowel is not really the disease, but merely an outward symptom of mischief going on within, and is further the useful and salutary effort of Nature to get rid of the irritating matter that is causing the mischief; and hence to stop the movements of the bowel, before the peccant matters have been got rid of, is a most dangerous step to take; so that no drug of the above description should on any account be given during the earlier stages of an attack of this sort. Next to this the matter of greatest importance is to give the irritated intestine rest by at once stopping the ordinary diet of solid food and substituting some mucilaginous preparation, such as milk thickened with a little arrowroot and taken cold. Where the attack is sharp, a few hours’ fast is by no means unadvisable, but must not, of course, be continued too long. Wherever possible, it is best for the patient to rest in bed, and if there be much abdominal pain a hot-water bottle placed against the pit of the stomach will afford great relief. In a large proportion of cases no other treatment than rest and avoidance of opiates is required. Avoid also alcohol in all forms, at any rate unless extremely diluted. If, however, the symptoms fail to moderate under this treatment, it is well to secure the removal of any irritating or poisonous matter that may remain in the bowel by the administration of a dose of castor oil, a full ounce for a grown-up person down to a teaspoonful for small infants. The great advantage of this drug is that besides acting as a safe and certain laxative, the oil itself forms a most soothing application to the irritated bowel, just in the same way as it does to the skin when that structure is scorched or otherwise inflamed. To treat an intestinal flux by the administration of a laxative may appear strange to the lay mind, but you need never fear to employ castor oil, however violent the flux may be, and in children especially, it is a good routine commencement of treatment for any looseness of the bowels. A good plan for getting down this remedy, which, it must be admitted, is usually most obnoxious to adults, is as follows. Select a wide, shallow drinking vessel, such as a champagne glass, and moisten its interior thoroughly with a teaspoonful of some strongly-flavoured spirit, such as gin, turning the glass about until all parts are wetted, then add a couple of tablespoonsful of water, and into the middle of this pour the oil, avoiding the sides, so that it floats separately, like the yolk of an egg surrounded by the white. If now the contents of the glass be swallowed as nearly as possible at a single gulp, the oil passes through the mouth and throat so completely surrounded by the spirit and water that its presence cannot be noticed. A tabloid containing 1⁄40 grain of perchloride of mercury should be taken shortly after, and after a lapse of three or four hours the disinfection of the contents of the intestine may be completed by taking a 10-grains tabloid of resorcin every four hours.
As a rule, under this treatment the yellow colour soon reappears in the motions and all symptoms disappear; but should the liver refuse to act, as is indicated by the continued absence of the natural yellow colour in the motions, it will be necessary to give a large dose of ipecacuanha—to get this drug down without setting up vomiting, requires a certain amount of preparation—as in smaller doses, it is one of the safest and most certain of emetics. It is best to give the dose the last thing at night, when the patient is naturally likely to be sleepy, and half an hour before it is given, a preparatory dose of a grain of opium should be administered. The patient should lie as quietly as possible, and after the dose (30 grains, or half a dozen 5-grain tabloids of ipecacuanha) all liquids should be withheld. It is also important to use as little water as possible to wash down the tabloids, as success in keeping down the drug depends mainly on the absence of any notable amount of fluid from the stomach; and this abstinence from fluids, as well as from food, should be continued until the next morning, when in all probability a copious bile-stained motion will show that the drug has taken its desired effect. As a rule, after this, two or three tabloids, containing 1⁄40 of a grain of perchloride of mercury per diem, for a few days, will suffice to maintain the action of the liver and to disinfect the bowel, but occasionally the medication with ipecacuanha may have to be repeated. Remember, however, that no drugs will be of much service in this disease without the greatest care in diet.
An Indian medical officer has generally a variety of institutions under his charge, and usually amongst them a prison, of which he is not only the medical officer, but also the military governor—a sensible combination of offices which might well be imitated elsewhere. Now, although dysentery is a disease which gives much trouble in Indian prisons, the writer did not lose a single one of his jail-birds from that cause for several years; and he imputes his success to the practice he made of at once relegating each case of dysentery to a solitary cell, where it was utterly impossible for the patient to obtain any other food than that ordered for him. When left in the general wards they could not be kept from obtaining more or less of the bread and vegetable curry that formed the ordinary diet of those not seriously ill.
Soups are rarely well borne in dysentery, and hence the diet must be restricted to milk foods, the milk being always rendered mucilaginous by the addition of a little arrowroot or gelatin, cornflour, &c. When there is much dyspepsia the milk may be given semidigested by combining it with one of the numerous pancreatised proprietary articles, such as Benger’s food. Afterwards a raw egg may be given beaten up with the milk or Benger’s food, and subsequently rice pudding and fish; but great caution is always required in resuming the ordinary diet, as the bowel always remains easily irritated for some time after the attack has subsided. Everything should be given cold (preferably moderately iced), and in small quantities at a time.
Diarrhœa.
Diarrhœa in tropical climates arises from much the same causes as dysentery, and like it, is very apt to be set up by chills to the abdomen; in fact, these diseases may be regarded, for the practical purposes of prevention and treatment, as different degrees of the same condition; the more serious disease being further complicated by concomitant affection of the liver. Heavy dosing with ipecacuanha will not, of course, be required in the milder disease, but otherwise its prevention and treatment may be regarded as the same, especially as in tropical climates, the mildest access of diarrhœa should always be respectfully dealt with, as it may easily develop into dysentery if neglected.
Hill diarrhœa is a peculiar form of chronic looseness of the bowels that is not uncommon in the Himalayas, and, I believe, in other elevated regions. Certain people appear specially liable to it, much in the same way as some are subject to hay fever, while others are never affected; and the proclivity is so marked in some persons that it is impossible for them to reside in such localities, and they are hence debarred from taking refuge from the fierce heat of the plains. We are not very clear as to its causation, though the disease is traceable in some places to the presence of finely divided mineral matter (mica) in the drinking water, and so may be guarded against by careful filtration of all water used for drinking or cooking. The climate of the hills, again, though pleasant enough, is during the rains even more treacherous than that of the plains—damp cold, alternating with warmth; but withal, as has already been remarked, the disease is mainly one of personal proclivity, and where the tendency is very marked the only course is to avoid residing in places where it is apt to occur. Should you, when travelling in the hills, be attacked with this malady, careful filtration of water and care in diet should be attended to, and a pill or tabloid containing one grain each of euonymin, blue pill and ipecacuanha may be taken at night; but should the trouble persist, no time should be lost in returning, if possible, to within range of competent medical assistance, as if neglected, the disease is apt to develop into a most troublesome condition known as sprue.
Infantile Diarrhœa
is terribly common in hot countries, and hence the least disturbance of this sort should never be neglected in young children. The rapid rise in the infantile death-rate that coincides with any approach to a tropical temperature in Europe, shows well how full of risk is a child’s tenure of life in latitudes where such temperatures are not the exception, but the rule. The liquid food, which alone is suitable to the infantile digestion, is perilously liable to decomposition when the temperature of the air rises much over 70° F., and, under such conditions, food which, to the nose and eye, shows no appreciable change, may yet be virulent with a poison as lethal in its effects as arsenic, and far more deadly, weight for weight. As a matter of fact, the poisons which may be generated in food subjected to high atmospheric temperatures, differ only from the most active of mineral poisons in their greater virulence, and to commence treatment in such cases with any agent that checks the action of the bowels ensures an unfortunate result with even greater certainty than if we were dealing with antimony or vitriol.
The first desideratum is to get rid of the supply of poison which has already been generated within the bowels, and the second to stop the fermentation which alone can generate the poison. To meet the first indication an unirritating laxative should be at once administered. When the symptoms are severe, one or two teaspoonfuls, according to the age of the child, of castor oil is probably the safest remedy, but in less violent disturbances a drachm of our old friend, Gregory’s powder, will be more appropriate. The laxative should be promptly followed by the administration of one of the intestinal antiseptics, amongst which I have a personal preference for 5-grain doses of resorcin; but β naphthol grs. ii., salicylate of bismuth grs. v., or perchloride of mercury gr. 1⁄64, if more readily to hand are equally valuable, and are, I know, preferred, one or the other, by practitioners according to their individual favourable experiences; but opiates of all sorts are always to be avoided as long as active mischief continues, though fifteen or twenty drops of paregoric or some other preparation of the poppy may possibly accelerate the cessation of obvious symptoms when the “causing cause” of the disease has been disposed of.
The germs that produce this intensely poisonous matter are quite different from those whereby milk “turns sour,” and the fermentation which produces it may go on some time without giving rise to changes obvious to the nose or eye. Hence, though it is no doubt possible for the germs to reach the stomach in other ways, as a rule the changes have commenced before the food is swallowed.
Diarrhœa is naturally rare in infants fed entirely at the breast, and from what has been said it will be clear that the surest protection against this terribly fatal malady lies in the avoidance of bottle feeding; for to carry out the latter safely in a tropical climate, would tax the resources of a skilled bacteriologist. It is, however, unfortunately the fact that European women residing in such climates are very often really unable to suckle their children, in spite of all the good will to do so; and when the supply is inadequate and has to be supplemented by artificial feeding there is little real gain, as the bottle, with all its dangers, must needs be used several times in the day. On this account, whenever the mother is unable to fully nourish her infant, by far the safest course is resort to wet nursing. I have met with people who have a sentimental objection to entrusting their child to a woman of another race; and are even capable of believing that the mental and moral qualities of their offspring may be affected by such a diet; but it should be needless to say that there is no foundation whatever for any such idea. Great care is of course necessary in the selection of the foster-mother, who should be young, healthy, and vigorous. Her own baby ought not to be much older than the one she is to nurse, while it is needless to say that she should never be permitted to nourish both infants together. It is also most important that she should be examined, and, if possible, selected, by a medical man.
When, however, artificial feeding is unavoidable, the most elaborate care as to the purity and cleanliness of the milk and all utensils that come in contact with it are required. In hot climates it is not enough to merely wash the bottles and jugs which are used. They should be boiled at least once a day, and in very hot weather, even each time after using. The simpler the bottle is in its construction the better, those with long tubes and elaborate screw stoppers being so dangerous that it is far better to resort to spoon feeding than be tempted to use one, even as a temporary expedient. The form of bottle which presents least dangers, because the most easily cleaned, is that in which the nipple is in one piece, with an elastic cap that is made to fit the mouth of the bottle, thus doing away with the necessity of any stopper or cork. Moreover, if the special bottle chance to get broken, it is generally easy to find some medicine phial, or other small bottle, over which the cap can be stretched and which serves equally well. Rubber will not stand repeated boiling, hence, when not in use the nipple should be always kept immersed in a strongish solution of boracic acid (10-15 grs. to the ounce) and rinsed before and after using in ordinary drinking water. In making the boracic solution, a sufficient approach to chemical accuracy may be made by placing an eggspoonful of boracic acid in a breakfast cup and filling up with boiling water.
Asses’ milk is probably the best substitute for an infant’s natural food; and failing this, goats’ milk is to be preferred to that from the cow. Whichever is employed, it is best to buy the animals and have them kept in one’s own compound, so that one can ensure, by personal supervision, their being cleanly kept and carefully fed. Before milking, the animal’s teats and the hands of the milker should be washed in boracic solution, which should be kept ready made up in a large earthen vessel (an Indian gurrah, for example).
A great drawback of cows’ milk as a food for infants in India lies in the fact that, whereas human milk has a distinct alkalinity, that of the breeds of kine indigenous to that country is often (in my own experience, always) rather strongly acid, even when freshly milked from perfectly sound and well-cared for animals.
Generally speaking, indeed, the acidity is so considerable that the amount of alkali contained in even twice its bulk of lime water, is quite insufficient to neutralise it. In place, therefore, of the conventional lime water, it is better to add about as much as will stand on a sixpence, of a mixture of equal parts bicarbonate of soda and citrate of potash, to each bottle. Of course, if you wish to be exact, you can get from your chemists some books of litmus paper which change to a redder tint when dipped into an acid fluid and become bluer when moistened with an alkali; and it is a good plan to test in this way, at any rate to commence with, in order to ascertain roughly the amount required for the milk of the particular cow that yields the milk. The citrate of potash, besides being for practical dietetic purposes an alkali, has the additional valuable property of preventing the milk, after it has reached the infant’s stomach, from curdling in large masses, as cows’ milk is apt to do unless treated in this way. Human milk, when curdled in the process of digestion, does so in small flocculi; and the tendency of cows’ milk to curdle in large masses makes it a frequent cause of dyspepsia as well as of diarrhœa. Whether or no the peculiarity of possessing a so strongly acid reaction is shared with the milk yielded by cows in other hot climates I cannot say. Whatever may be the source of the artificial food, it is needless to remark that it should be sterilised by means of one of the numerous appliances now sold everywhere for the purpose, and that care should be exercised to guard against chill to the abdomen.
The prevention of infantile diarrhœa is in fact purely a question of guarding against impure and unsuitable food, and though the same is no doubt also true for more temperate climates, precautions which may be sufficient in an English summer, break down at once in a moist heat of 90° in the shade.
Should, however, in spite of all precaution, the disease appear, steps should at once be taken to get rid of the food that is fermenting within the stomach by administering a teaspoonful of castor oil, and if any obviously large proportion of the oil be thrown up within half an hour of taking the oil, give another half teaspoonful. The milk given should be much more diluted than usual, and if it obviously continues to disagree, as evidenced by continued sickness after the bottle, it should be pancreated by means of Benger’s food, which will often be kept down where the simply sterilised milk is rejected. If, however, milk in any form prove unsuitable, meat juice may be substituted for a few hours.
Meat juice is made by mincing raw lean meat, sprinkling lightly with salt, and adding just enough blood-warm water to cover it. Place the mixture aside in a covered jug in the sun for two hours and then place the pulpy mixture in a clean cloth and squeeze out the juice into a basin by wringing the cloth. Before administration, a sufficiency of sugar to make the mixture palatable should be added.
Another very useful food, as a temporary substitute for milk, when the latter disagrees, is egg albumen. To prepare this, beat up the white of a small egg with enough cold water to make a bottle, add just enough sugar to perceptibly sweeten, and let it stand till the froth produced in the beating has settled. Should these novel delicacies be refused by the infant, the addition of even a teaspoonful of milk will often lend sufficient of the desired flavour to induce the child to take it. The egg albumen should always be given cold, as even warming the bottle by placing it in hot water might easily coagulate a little of the albumen and so convert an exceptionally bland food into a very dangerous and indigestible material. After the oil has acted, about 5 grains of Gregory’s powder may be given once or twice a day, and if the natural yellow of the child’s napkins be not rapidly recovered a grain of grey powder should be added.
The course of infantile diarrhœa is often appallingly rapid, so that all may be over with the little sufferer in a few hours, and on this account there should be no delay in obtaining medical assistance, even on the appearance of slight symptoms of the kind, wherever such help is at hand.
Plague.
Strictly speaking, this terrible scourge cannot be said to be in any sense a disease peculiar to warm climates, for the one climatic condition that appears to check the course of epidemics of this disease is extreme heat, which always moderates their virulence as long as it lasts. In reality, it is a disease of low civilisation; and appears to be practically incapable of attaining any serious spread amongst people of European habits. During the terrible recrudescence of this disease, which, for the last decade, has been ravaging the semicivilised world, although repeatedly introduced, it has never succeeded in seriously establishing itself in any European town. Even the admittedly backward sanitation of Spanish towns appears to be too advanced to admit of the spread of plague, and, what is more remarkable, the European portion of the population of plague-stricken Eastern towns has remained practically unscathed, while the indigenous population have been dying around them in their thousands. When first the disease invaded India there was naturally a good deal of alarm amongst the European population of Bombay, but nowadays the official, commercial, and social life of the European community goes on unmoved, even at times when the disease is doing its worst—and is so assured of its own immunity that timid ladies out for their evening airing will scarcely turn their head as the bodies of the plague-stricken are carried past them on the way to the burning ghaut. Perhaps this immunity may be to some small extent a question of race, but the main determining cause is undoubtedly difference of habits of life, as natives who have adopted European habits share in it.