Hitherto, these general observations on amputation have regarded the operation by flaps only; the circular method has not been mentioned. The reason is, that the circular amputation has been, it is hoped, in a great measure abandoned in this country. And its inferiority to the method by flaps is so obvious, and so generally acknowledged, that detail of the different steps of the operation is, I conceive, here altogether unnecessary. It is more tedious in performance, more painful to the patient, does not afford so good a covering for the end of the bone, and consequently not so convenient and useful a support for an artificial limb, and the cure of the wound is protracted. The stump is almost always conical, the end of the bone is, ultimately at least, covered only by integument, and from even very slight pressure this is apt to ulcerate; exfoliation of the bone follows to a greater or less extent, or unhealthy nicer of the soft parts continues, along with caries of the bone, and partial death of its surface; and at length it becomes necessary either to perform a second amputation or to curtail the length of the bone. It may sometimes succeed tolerably well when there is but one bone: when there are two, it is altogether inadmissible. In very muscular limbs, when amputation is demanded on account of destruction of the bones and joints, with laceration of the soft parts, as when the patient is not required to have pressure made on the stump, it suits well to make the flaps of integument only, and to cut the muscles short, as will be noticed more fully afterwards. The advocates for the circular amputation, my excellent friend Sir George Ballingall, and others wish it to be believed, (and this is their main argument,) that the exposed surface of the flaps is much greater than that in their favourite method. Some of the philosophers of the Modern Athens have been appealed to, and have measured, it is said, the area of the one and the other, and given their verdict in favour of the round about incision. The accompanying drawings from nature, and the corresponding diagrams, speak pretty plainly in favour of the other method. In the first there is a cone formed by the cut skin and muscles, with a corresponding hollow and ragged cavity; and the second set shows two smooth, nearly triangular surfaces, which the said philosophers may measure and report upon at their leisure.
Various accidents and diseases require removal, either primary or secondary, of the fingers, or of parts of them. Amputation is most easily accomplished at the articulations, and ought therefore always to be performed at these points, when the circumstances of the case permit. The last phalanx may require removal either on account of severe injury, or from incurable disease, as onychia maligna, necrosis, caries, &c. The operation is one by single flap, and may be conducted in one of two ways. The doomed phalanx is grasped, on its anterior and posterior aspects, by the fore and middle fingers of the left hand; and the articulation is flexed almost to the full extent, in order that incision into it may be facilitated. A straight, narrow, and sharp-pointed bistoury is carried in a semicircular sweep over the back part of the joint, so as to divide the integuments, and open completely the articulating cavity. The remaining ligamentous investments of the joint are divided by one or more additional touches of the knife, so as to loosen the base of the phalanx. The fingers of the left hand are then changed from the fore and back parts of the phalanx to its sides, the edge of the knife is passed behind the base of the bone, and the surgeon, by carrying the blade forwards and downwards, forms a flap of sufficient dimensions to cover the wound, and removes the offending part. There is seldom any trouble from hemorrhage; no ligatures are required. The flap is turned up so as to form a cushion over the exposed surface of the middle phalanx, and is retained so by the adhesive composition formerly mentioned, or by one or two turns of a linen bandage. The other method of operation is the reverse of the preceding. The joint is extended, the bistoury is made to transfix close to the joint and at its anterior part, and by then carrying it downwards and forwards, as before, a similar flap is formed; this is retracted by an assistant, and with one sweep of the knife the articulation is divided from before backwards. By either method the flap is the same. By similar procedure the amputation at the middle articulation is performed.
It is sometimes an object to save as much as possible of the proximal phalanx, when amputation is rendered necessary by disease of the middle articulation, or of the distal extremity of the bone. In such cases, two semicircular flaps are made by cutting from without, either on the lateral, or on the thenal and anconal aspect, and the bone is divided either by a small saw or by the cutting pliers. The flaps are retained in apposition, and the bleeding arrested by bandaging.
Amputation at the proximal articulation is also performed by double flap. In the previous operations an assistant steadies and supports the hand; in this he has likewise to bend the rest of the fingers, and to separate as widely as possible those neighbouring to the one about to be removed. The operator seats himself before the patient, grasps the finger so as to manage its movements with the left hand, and holding the knife perpendicularly, with its point upwards, lays it over the knuckle, and carries it obliquely upwards so as to open that side of the articulation. He then pushes the finger towards the opposite side, and with the point of the knife completes the loosening of the articulation; for this the blade of the instrument should never be employed, otherwise the integument will be cross-cut and mangled. After separation of the base of the phalanx by the point, the blade is passed behind, and carrying it downwards and outwards, a flap is formed similar to the first—both proportioned to the size of the wound which they are to cover, and the bone which they are to protect. The fingers may also be removed by the oval method, as described and delineated in the Practical Surgery. The flaps are retained in contact by bringing the neighbouring fingers towards each other. This also suffices, in general, to suppress the bleeding, but sometimes one or both digital arteries require ligature. At first, cold cloths are probably the best applications, with the view of stopping the oozing, and warding off inflammatory action. Vascular excitement is very apt to follow this amputation, when performed for disease of the finger, as after neglected or severe whitlow; the soft parts in which the incisions are made are generally infiltrated and condensed, and prone to inflammation. The surface around is red, tense, and shining, on the second or third day; the back of the hand, the palm, and perhaps the forearm, are then involved in inflammation of the surface, and infiltration of the cellular tissue; and in all probability, free incisions, followed by poultice and fomentation, will be necessary to restore the parts to quietude. Such consequences are to be guarded against as much as possible, by attention to the system, and by avoiding all irritating dressing.
The phalanges of the thumb are removed in the same manner as those of the fingers. Amputation of the metacarpal bone is accomplished thus. The thumb is grasped by the fingers of the left hand, and so managed. The bistoury, held in the same manner as for amputation at the proximal articulation of the finger, is placed with its point on the web betwixt the thumb and forefinger, and carried in one sweep rapidly upwards in a slightly oblique direction, till it is stopped by the os trapezium. The point is used to effect disarticulation, the member being at the same time pushed steadily outwards; the blade is then placed behind the base, carried downwards close to the side of the bone, and is not to be brought out till sufficiently low down for forming a flap to cover the whole wound. The flaps may be formed otherwise, and much more handsomely, by transfixion of the ball of the thumb, as shown in the Practical Surgery, p. 360. After arresting the hemorrhage, the flap is laid smoothly down, and retained in its proper position by bandage or slips of the adhesive plaster. The metacarpal bone of the little finger is removed by the same method of incision as for the thumb.
In amputation of the fingers, the incisions sometimes require to extend beyond the proximal articulation, on account of disease having involved that part; in other words, it may be necessary to remove more or less of the metacarpal bone along with the finger. The method of incision will vary according to the extent to which the bone is diseased. When the operation is required for disease of merely the distal extremity, the incisions are made in the same form as for amputation of the joint, only they are on each side sufficiently high to be beyond diseased bone. They may either be made from below upwards in the usual way, or be commenced at their highest point on the dorsum of the metacarpal bone. After the soft parts have been separated from the bone, by a few touches of the knife after formation of the principal incisions, removal is completed either by the cutting pliers or the metacarpal bow-saw—the former I have found the more convenient instrument. It is applied perpendicularly, and should always have its smooth surface in contact with the part to be retained, otherwise the cut part will be rough and irregular. Section is completed more rapidly than by the saw, and, by attention to the above precaution, the stump is equally smooth, if not more so. The wound is brought and retained in contact by approximation of the fingers. But in taking away any considerable portion of the metacarpal bone, it is of importance to preserve the palm uninjured. With this view, the knife is entered over the centre of the bone on its dorsal aspect, above the diseased part, and carried straight downwards till near the articulation, when it is made to diverge for the formation of lateral flaps; the integuments in the track of the longitudinal wound are then dissected backwards, so as to expose the bone completely, and the bistoury is passed round the bone throughout its whole extent, the edge being kept close to it,—in order that the soft parts may be separated, and that without unnecessary width of wound or implication of the palmar arches and branches proceeding from them. Then the bone is clipped at the proper point by the cutting pliers; or the section of the bone may be performed before separation of the soft parts from its under surface, as, by raising the cut end, this part of the operation may be facilitated. Here the metacarpal saw is inapplicable.
Before quitting this part of the amputations, it may be observed, that no good can result from taking away a metacarpal bone and leaving a finger, or from removing a proximal phalanx and leaving the distal. The parts so left can be of no use, they have no support, and the muscles cannot act upon them: they must prove an incumbrance, and as such will either form the subject of a second amputation, or remain a proof of the unsuccessful result of the first.
Amputation in the forearm, may be necessary at various points, on account of accident or disease, but should never be resorted to, in either case, so long as part of the hand can be saved. The preservation of even a small portion of this useful member, even of one finger or a part of one, is of great importance to the patient. When, however, this is hopeless, all must be removed; and, if the wrist be sound, amputation may be performed at that joint. Hitherto, no mention has been made of the temporary suppression of bleeding, for in the amputations detailed there is scarcely ever any necessity for adopting such measures; but in those of the forearm and arm, a steady assistant must be placed ready to compress the humeral artery as soon as the incisions are commenced; in the case of the forearm, the pressure is made on the lower portion of the artery; in the arm, the point of pressure will necessarily depend on the point of removal. The patient may be either seated or recumbent. One assistant compresses, another steadies the limb in the supine position. The surgeon holds the hand in his left, standing on the inside of the right limb, and on the outside of the left. Suppose the right wrist is to be operated on,—the end of the ulna is felt for, and at that point the knife is entered, and drawn across the wrist on its dorsal aspect in a semilunar direction, the convexity of the curve of course pointing towards the fingers. The joint is opened by retracting and dissecting back the flap so formed; the knife is then passed behind the scaphoid and lunar bones, which are exposed and turned out by division of the ligaments, and by rapid and gentle sawing motion downwards and forwards, a flap of sufficient size is then formed on the palmar aspect. The dorsum of the hand may be so diseased or injured as not to afford sufficiency of sound parts for a posterior flap; in such circumstances the anterior must be made proportionally large, that it may alone cover the ends of the bones. After suppression of the bleeding, the flaps are approximated by one or two points of suture; these are afterwards removed, and their place supplied by the adhesive plaster.
Amputation, at any point between the wrist and elbow-joints, requires, in all, the same method of incision, but the nearer to the elbow the better is the stump; at the wrist the flaps are composed principally of integuments and tendons, and the cushion so formed for the bones is very inferior to one of muscle. Compression is made and the limb steadied as before; the surgeon with his left hand grasps the wrist, and places the forearm in the middle state between pronation and supination. In the right forearm, the knife, held perpendicularly, is entered over the centre of the radius, and its point, after reaching the bone, is inclined inwards so as to pass round it; transfixion is then made, the knife passing close to the palmar surface of the bones, and emerging at a point opposite to its entrance; and then by rapid motion downwards and inwards, a proper flap is formed. The instrument is again introduced over the radius, at a little distance from the upper part of the first wound, and passed on the opposite side of the bones, emerging also in the first incision and at a similar point; another flap is made. These are retracted, the knife is swept round the bones, and passed freely between them, to divide the remaining muscular substance, and after this has been completed, the saw is applied. During the sawing it is well to preserve the limb in the same position as during the incisions, and to apply the instrument perpendicularly; thus both bones will be divided at once, and the risk of splintering diminished. In transfixion, great care is required that the point of the knife pass across, not between, the bones, and with this view a slight change of position is useful; during the transfixion for the inner flap, the surgeon, as soon as he feels the knife rounding the radius, rotates the forearm gently inwards, and in transfixing for the outer flap similar rotation is made outwards. In this situation, and others where the soft parts are less thick in one aspect than the other, it is by much a preferable plan to make a flap first, by cutting from without inwards, as already described in regard to the wrist, and then to transfix for the formation of the second flap. This is delineated in the Practical Surgery, p. 367. Sometimes slight difficulty is experienced in tying the interosseal artery. The flaps are brought together, and treated in the way already mentioned.
In all amputations of the upper extremity, it is of importance, and indeed a rule scarcely to be departed from, to leave as much of the limb as possible; for here the longer the stump, the more useful is it to the patient. In accordance with this maxim, amputation at the elbow-joint may be required, when either disease or injury extends too high for amputation in the forearm, but not too high for the formation of an anterior flap over the joint. The limb is steadied in the supine position, compression being made near the middle of the humeral artery; the knife is passed horizontally across the condyles close to the bone, and brought downwards and forwards to a sufficient extent for the production of a flap, which is alone to form the protecting cushion. The joint is then cut through, the knife is passed down till obstructed by the olecranon, and with one sweep a semicircular incision of the posterior integument is made. All soft parts in this line are divided, and then the saw is applied to the olecranon process. This amputation is easy, rapid, and beautiful in execution; and, when the flap is sufficiently large,—as it always may be, for there is no want of soft parts in front,—the stump is well formed and useful. The flap is laid down, and attached by suture to the integument posteriorly; in due time the adhesive dressing is applied. The circumstance of a secreting surface forming the stump does not seem detrimental, either here, or in the wrist-joint. The synovial fluid soon ceases to distil, and union is not interrupted by it. There is no necessity for scarification, or scraping the cartilage, with the view of hastening cessation of secretion and granulation of the surface.
Amputation of the arm is performed by the formation of lateral flaps, at any point below the insertion of the deltoid muscle. Compression is made on the upper part of the humeral, or on the axillary artery. The limb is held well separated from the side; and care should be taken that, when so raised, its height be convenient to the operator. The knife is entered perpendicularly to the shaft of the bone, passed fairly down to it, and then inclined along its side; the operator now grasps the limb below the line of incision with the left hand, and pulls the muscles towards him—it is supposed that the right arm is being amputated, the surgeon standing on the inside, and an assistant supporting the forearm—and then completes transfixion, inclining the handle of the knife towards himself, in order that its point may pass round the bone and emerge at as distant a point in the circumference of the limb as possible. By a rapid sawing motion, downwards and inwards to the proper extent, the inner flap is formed; and by attention to the grasping of the muscles and the inclination of the knife, its base is so large as to admit of the more easy performance of accurate transfixion for the outer—that is, the instrument is more easily brought through the same incision. The assistant seizes the extremity of the inner flap as soon as formed, and retracts it, but only to a slight extent; it is simply held out of the way. If it be pulled backwards, as in retraction during sawing, the formation of the second will be much impeded. The knife is again entered about half an inch below the commencement of the first incision, and by inclining the handle the point is brought round the bone, and made to appear on the opposite side also in the first incision; this is facilitated by pulling the soft parts outwards with the left hand. Then the outer flap is completed. The knife is swept rapidly round the bone, so as to expose it completely at the upper part, the assistant at the same time retracting the flaps fully. The saw is applied, the arteries tied, the flaps approximated, and the operation completed.
In performing the second transfixion, the reason why the knife is entered lower than in the first, is, that cross-cutting of the corners of the wound is thereby avoided. For a long time I was surprised and annoyed to find many stumps present an unseemly cross-cutting of the integument at the upper parts, particularly after approximation of the flaps, although the incisions seemed to have been made smoothly and accurately. It is occasioned by the sawing process for making the second flap, and when this is commenced at the same height as for the first, irregularity of incision at the upper part is unavoidable. The precaution, however, of making the second transfixion considerably lower than the first I have found quite effectual. The disparity between the bases of the flaps is readily and quickly remedied, after their formation, by a sweep of the knife upwards on the lower side.
Irritable and painful stumps are more frequently met with after the amputations of the arm and forearm than any other. The occurrence, however, is less common than formerly, and this may be fairly attributed to the improvements in the operation—to the method by flaps having superseded the circular, and nothing but the arteries being surrounded in ligature. Still the affection is occasionally met with, and there can be none more painful and troublesome. Generally, no obvious cause can be found for the attack of this malady; but in some of the cases there would seem to be a constitutional and innate tendency, as it were, towards this irritability of the cut and bulbous extremities of the nerves—as in the following case:—A gentleman, aged 53, underwent amputation of the thumb, in consequence of laceration of the hand. Amputation was very soon afterwards performed at the middle of the forearm, on account of hemorrhage and infiltration of the hand, after fruitless attempts to secure the arteries. After cicatrisation of the wound, he complained of great pain in the stump, and in the situation where the tourniquet had been applied. Amputation of the arm was then performed, but the stump was not well made. The pain returned, and he applied to me, with the view of again submitting to amputation. It was performed nearer to the shoulder-joint, and in order to guard against recurrence of the disease, the nerves were laid hold of, pulled outwards, and cut across as high as possible. The patient was relieved of many of his sufferings, and continued tolerably comfortable for nearly two years; again, however, the painful symptoms have returned, though in a slighter degree. On examining the removed stump, all the nerves, particularly the musculo-spiral, were found greatly enlarged in their extremities, and intimately adherent to the cicatrix and the ligamentous covering of the rounded extremity of the humerus. More desperate operations have even been performed to free patients from irritable stump. The lower limb has been hacked off bit by bit, even to the coxo-femoral articulation, without much, if any, relief. Such operations are hardly warrantable.
Amputation at the shoulder-joint is more frequently required for accident than for disease. It has always been the custom to trust for suppression of bleeding, during this operation, to the hands of an assistant; and when the method has been found effectual in the case of the large axillary artery, why should it be objected to, on the score of inefficiency, in the minor amputations? particularly when it is evident, putting efficiency out of the question, that it is preferable to compression by the tourniquet, or any other circular apparatus;—more quickly applied and relaxed; less painful, less formidable; always ready, and independent of the instrument-maker. The compression is made above the clavicle, so as to secure the subclavian, where it passes over the first rib. The thumb of a steady assistant is placed deeply into the cavity of the lower triangular space of the neck, immediately above the first large sinuosity of the clavicle. The pressure thus made is quite effectual; but as it requires to be firm and uniform, and as there is always a risk of the thumb giving way from exhaustion, it is better to interpose some mechanical contrivance when the assistant is either diffident or inexperienced. The best apparatus for this purpose is a common door-key. A bit of lint or cloth is wrapped round the handle, and this part is then pressed down on the vessel. As in other amputations, the pressure is not commenced till the knife is about to enter.
The flaps may be double, on the outer and inner aspects, or one may be made sufficiently large to cover the whole wound. The patient is seated on a chair, and secured by a person placed behind. The arm is raised a little from the side, and supported by an assistant. Two oblique incisions are made, commencing high on each side of the shoulder, and converging gradually till they meet near the insertion of the deltoid. The triangular flap, so marked out, is dissected rapidly upwards, close to the bone, and kept raised by an assistant. The person supporting the arm then uses it as a lever, carrying it downwards and backwards; the joint, thus made more palpable, is cut into by a semicircular sweep of the knife across it; the head of the bone is now dislocated, and the rest of the capsule and fibrous tissue exterior to it divided; the blade of the knife is insinuated behind the head of the bone, and carried rapidly through the remaining soft parts. In no amputation can I conceive any necessity for suspending the incisions, in order to secure vessels, provided the pressure is well applied, and the knife used dexterously. Here very little blood should be lost. The vessels divided in the formation of the flap are small, and the axillary is not cut till the incisions are nearly completed; as soon as the limb has dropped, the surgeon places his finger on the mouth of the artery, and then applies his ligature as quickly as possible; the pressure may now be removed, and the minor vessels secured leisurely. The flap covers the wound completely, and is easily retained.
Or two flaps may be made by transfixion. In operating thus on the right limb, the surgeon, standing in front of the patient, enters the knife a little below the point of the acromion, passes it across the outer aspect of the joint, and by inclination of the handle outwards, makes its point to appear on the inside of the outer margin of the axilla; by carrying it downwards and outwards to a sufficient extent, the outer flap is formed. This is immediately elevated by an assistant, and then the arm is pushed upwards, and across the chest, so as to render the joint more accessible; the ligaments are cut, the bone disarticulated, the knife passed beyond its head, and placed with the edge parallel to the shaft of the humerus, and the arm restored to its former position; the inner flap is then made by carrying the instrument downwards and inwards. In the left limb, the knife is entered on the inside of the outer border of the axilla, and brought out below and in front of the extremity of the acromion, reversing the order of the former incisions; after the outer flap has been so formed, the joint is cut across, the knife passed beyond the head of the bone, and the inner flap made as before.
Accidental injury, as already stated, is the most frequent cause for amputation at this part, and this will always influence the method of incision. There is nothing peculiar in the after-treatment of the stump. But it ought always to be remembered, that the operation is one of great severity; that a large part of the body has been suddenly removed; that, consequently, there is risk of the mere shock being dangerous, and of an untoward constitutional condition supervening—and, therefore, the after-attendance should be zealous and careful.
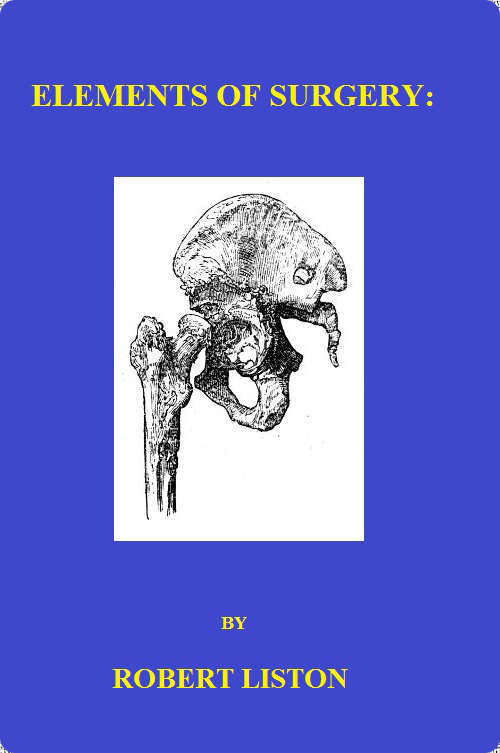
The phalanges of the toes are removed in the same way as those of the fingers. This latter operation may be required on account of bad onychia, large exostosis or injury. This and the other must also be removed on account of diseased bone, such as here represented with affection of the interposed joint. The osseous shell formed by the enlargement of the original tissue encasing a segmentum is well represented. In the amputation at the proximal joint, it is to be recollected that the extremity of the metatarsal bone lies more removed from the web of integument betwixt the toes than the metacarpal bone does from that of the fingers. The incision upwards, therefore, requires to be deeper; but in other respects the operations are precisely the same.
In amputating at the proximal articulation of the great toe, there is often a difficulty in obtaining a sufficient covering for the wound, on account of the presence of the sesamoid bones, and the general bulging of the heads of the bones. The knife is entered on the dorsum of the metatarsal bone, about half an inch above the joint, and then inclined to each side, marking out lateral flaps of considerable length; these are then reflected,—in making the outer, the instrument being dextrously passed round the sesamoid bone,—and the disarticulation completed.
In removing the great toe, along with the metatarsal bone, the bistoury is entered over the articulation of the metatarsal bone with the tarsus, and carried straight downwards, along the centre of the dorsum of the bone, till near its extremity; it is then inclined to each side, in the manner described for amputation of the metacarpal bones. The integuments are dissected off on each side of the longitudinal incision, and the knife run up along the inside of the bone, till stopped by the tarsus. The surgeon now presses the toe outwards, so as to assist the disarticulation; and after this has been completed, the bistoury is carried downwards, close to the outside of the bone, and not brought out till past the lower articulation. The external flap thus formed is then laid accurately down, so as to cover the wound, and retained. The preferable mode of making the flap, so as to expose the metatarsal bone for division or disarticulation, is well illustrated in the Practical Surgery, p. 375. The entire bone must be removed in such cases as that here sketched. In cases in which the shaft is comparatively sound, and the disease is principally seated in the articulation with its distant extremity, the shaft may be divided with the cutting forceps at a point sufficiently removed from the disease. The operations on the other metatarsal bones are the same as those on the metacarpal. They may be removed, either entirely or in part, along with the corresponding phalanges, by operative procedure similar to that practised on the hand.
Sometimes disease of the foot is not so extensive as to require or justify removal of the whole organ; the metatarsal bones are not involved throughout their whole extent. The same remark applies to injury by accident. In such circumstances, amputation is performed at the articulation of the metatarsal bones with the tarsus. The operator first ascertains the exact site of these joints, and then transfixes the foot at that point, passing the knife close along the plantar aspect of the bones; carrying the instrument downwards, a sufficient flap is formed to cover the stump, or a semicircular flap may be made and reflected by cutting from without inwards. The integuments on the dorsum are then divided in the line of articulation, the joints divided successively, and the parts removed. The flap is raised, adjusted, and retained. In dividing the articulations, it is to be recollected, that the base of the second metatarsal bone, reckoning from that of the great toe, is lodged considerably higher than the others; and, therefore, the knife must be inclined upwards at that point, or else the use of the saw is requisite. The stump thus formed proves exceedingly useful: the subsequent lameness is not great; the heel and tarsus compose a very efficient support for the weight of the body, and the flexion is unimpaired; by attention, too, the deformity may be in a great measure concealed. In short, the surgeon who amputates above the ankle, for disease or injury not extending to the articulation of the metatarsus with the tarsus, is guilty of a serious error.
The disease may reach higher than is compatible with the preceding operation, and yet it may be possible to save the heel. In such cases amputation is performed in the articulations of the os calcis with the os cuboides, and of the astragalus with the os naviculare. The plan of the incisions is the same as that for the operation at the bases of the metatarsal bones.
No amputation is more frequently performed than that of the leg. Operation near the ankle is inadmissible; sufficiency of soft parts, for the protection of the stump, cannot be procured lower than the calf. Incision is completely limited to two points, either immediately below the tuberosity of the tibia, or in the bellies of the gastrocnemii. The former is the situation to be preferred in hospital practice, and amongst the lower orders generally; the latter is suitable to the better classes of society, that is, to those who can afford to purchase an expensive artificial support. The amputation below the tibial tuberosity being the most frequently required, will, with propriety, be described first. Suppose the right leg is to suffer:—The operator places himself on its inner side, according to the general rule formerly inculcated, and grasps the lower part of the limb with his left hand, an assistant supporting the foot at a proper height, and controlling motion. The knife is entered over the fibula, on its outer aspect, and carried upwards along that bone for an inch and a half, or two inches; it is then brought across the limb in a semilunar direction, the convexity of this incision pointing towards the foot, and after reaching the inner and lower part of the tibia transfixion is performed, the instrument being pushed along the posterior surface of the bones, and made to emerge at the upper part of the fibular incision. By then carrying the knife downwards, a posterior and larger flap is formed sufficient to cover the stump. All this is effected by uninterrupted sweeps of the knife, that is, without ever removing the point or edge from the track of incision. The integuments on the fore part are then dissected upwards a little, by a few touches of the knife, so as to form a small semilunar flap; at this part of the operation there is no necessity for laying down the knife and using a bistoury. The muscles in the interosseous space are then completely divided, and the knife swept round the bones to detach the soft parts still uncut. The saw is applied, either in a horizontal or perpendicular direction; I prefer the latter for reasons already assigned. The vessels are secured, and there are generally but three—the popliteal, and two sural. I now generally aim at cutting the vessel before it divides, and seldom fail in doing so. There is then possibly the popliteal only requiring ligature, and there is less chance of secondary hemorrhage. This has occurred, so as to prove fatal at a considerable period after the operation, in consequence of the posterior tibia being cut close to its origin, and no clot having formed in it. Before adjusting the flap, it is well to assist nature in rounding off the end of the tibia, and thereby prevent danger to the integument; with this view the sharp anterior ridge of the bone is cut away and rounded off by means of the pliers. This must be done sparingly if at all, and with great caution. The nipped surface is liable to exfoliation, or the medullary web is apt to be injured, and this is inevitably followed by more or less death of bone. To some the fibular incision may appear unnecessary; but I have long practised it from conviction of its advantage. It is an excellent mark for transfixion, and assists greatly in preventing entanglement of the knife betwixt the two bones; besides the soft parts in this situation must be divided at one or other step of the operation, and hence the procedure cannot be objected to on the ground of causing unnecessary wound. In operating on the left limb, there is not the same danger in transfixion, and consequently so long a preliminary incision on the inside is not requisite; in other respects the steps of the operation are the same as for removal of the right. In muscular subjects two semilunar flaps had better be made, one from the anterior aspect of the limb, the other from the posterior, the muscles being cut short in the ham, and the incision made to reach the popliteal artery.
It has been proposed to excise the head of the fibula after formation of the flap, instead of sawing it across at a corresponding point with the tibia. At one time I put this modification into extensive practice, with the effect of improving the appearance of the stump very considerably; but in several cases, untoward consequences took place. Discharge of synovia occurred on the second day, followed by very profuse suppuration, which proved of long continuance, and very exhausting; in more than one case, the joint became anchylosed, rendering the stump very inefficient as a means of support, in consequence of being fixed at an inconvenient angle; and one patient sank, exhausted by the profusion of the discharge. I then found, from repeated examination of the parts on the dead subject, that it was very difficult, nay impossible, to excise the head of the bone without dividing the capsular ligament, and wounding the synovial pouch, or opening a bursal cavity, beneath the popliteus muscle, communicating with that of the knee-joint. It is scarcely necessary to add, I have since wholly abandoned this method of operation.
It has been already observed that high amputation of the leg is preferable amongst the working classes. The limb is of much greater use to the patient than were the stump longer; he is able to follow his occupation with greater ease and security, and at less expense, by resting on the knee, than by using the artificial limb applied to the middle of the leg. The wealthier patient, however, can afford a more expensive support, and a less efficient, though more handsome continuation of the limb suffices. In such circumstances, amputation is performed at the middle of the leg; after cicatrisation, the artist supplies an artificial support resembling the natural limb; and thus the motion of the knee is preserved. The same directions apply to this operation as to that immediately below the knee.
In amputation of the thigh, the same method of incision is followed as in amputation of the arm. But, according to the point of removal, the direction of the flaps varies. If in operating high in the limb the flaps be made laterally, there will be imminent risk of the bone protruding through the upper part of the wound; for the patient uniformly raises the stump towards his abdomen. No antagonist muscular power is left to oppose the action of the muscles inserted into the trochanter minor, and the elevation of the stump is involuntary: it always occurs to a remarkable extent in young persons. On this account, anterior and posterior flaps are here far preferable to the lateral; for then the more the stump is raised, the better is the end of the bone covered—the anterior flap folds over it. Transfixion is therefore made horizontally; and the posterior flap should be a little longer than the anterior. But in the lower part of the limb, lateral flaps are not only not liable to the same objection, but preferable to the anterior and posterior. In the neighbourhood of the knee-joint, the soft parts consist almost entirely of ligamentous tissue on the fore and back part, and proper cushions can be obtained only from the sides. Transfixion is therefore made perpendicularly. Thus the bone will be well covered by parts likely soon to adhere; and there is no risk of protrusion, for muscles are left to counteract the elevators, and there is sufficient lever in the limb whereby to control its motions. And it may be here mentioned, that after all amputations, when startings of the muscles are not only painful, but disturb the position of the stump, the limb should be bound down by a broad band, passed across it a short way above the wound, and fastened firmly at each end to the bed or pillow; at the same time anodynes are to be administered. I have long since come to the conclusion that the femur in amputation should not be sawn lower than its middle; the method by anterior and posterior flap is therefore the only one applicable.
Amputation at the hip-joint is deservedly ranked amongst the most formidable operations in surgery. It ought, therefore, never to be performed but as a last and necessitous resource for the salvation of life. At the same time, when necessity for it is obvious and acknowledged, and no other means can be of any avail, hesitation and delay should never take place; otherwise the last and only chance of saving the patient will pass away, and the operation, when at length performed, will but hasten his exit from this world,—and besides inflict an injury to science, by intimidating practitioners, and affording subject of reproach and ridicule to the thoughtless and uninformed part of the public. I prefer the formation of anterior and posterior flaps,—as follows:—The patient is placed recumbent on a firm table, his nates resting on, or rather projecting a little over, the front edge. The sound limb is separated from the one to be removed, and held aside by an assistant. Or it is secured to the foot of the table by a towel, the necessity for an additional assistant being thus done away with, and more freedom in his movements afforded to the operator. Indeed, in all amputations of the lower extremity, this is the preferable method of fixing the sound limb. The other limb is supported by an experienced and intelligent assistant, who understands, and is able to perform, the movements to facilitate the different steps of the operation. The compression is intrusted also to an experienced and steady assistant, who, standing by the patient’s side, presses firmly with one or both thumbs on the femoral artery, where it passes over the pubes; and in this more than in any other operation should the pressure be delayed till the instant of incision, for otherwise the blood lost in the limb will be immense. Transfixion, by a knife proportioned in size to the dimensions of the limb, is made horizontally, the instrument being passed in a somewhat semicircular direction, so as to include as much of the soft parts as possible; an anterior flap is made by cutting downwards. During the passage of the knife across the joint, the assistant rotates the limb a little, so as to facilitate the bringing of the instrument out with its point well inwards; in the left limb the rotation will be inwards, in the right outwards. After formation of the flap, the assistant abducts forcibly, and presses downwards; the joint is opened, the round ligament cut, the capsule divided, and the blade of the knife placed behind the head of the bone and the large trochanter; the posterior flap is then made rapidly. After transfixion for the superior flap, and when the sawing motion downwards has advanced but a little way, the compressing assistant shifts one of his hands into the incision, immediately behind the back of the knife, and so obtains a firm grasp of the femoral artery previously to its division. He retains this hold, at the same time retracting the flap, during the rest of the operation. As soon as the limb has been separated, the surgeon secures the vessels on the posterior flap, partly by his fingers, partly by compression with a large sponge, and ligatures are applied as quickly as possible. The femoral is secured last; for, as long as the assistant retains his hold, hemorrhage from it is not to be dreaded. Thus, when both surgeon and assistants are quick and cool, the operation may be completed with the loss of much less blood than might be expected. I have had occasion more than once to perform this operation, and thus speak from experience. In cases of accidental injury requiring this operation, the lever use of the limb must frequently be wanting; and in such cases, too, the parts may be so injured as not to afford flaps anteriorly and posteriorly. In these circumstances, the surgeon must be guided by experience and judgment in adopting the mode of procedure which appears most applicable; in ordinary cases the operation above detailed appears the preferable.
Excision of diseased portions of bones, is practised occasionally with the view of removing a source of irritation and exhaustion from the system, without sacrifice of a limb. When the operation proves successful, the beneficial effect on the general health is as remarkable and rapid as after removal of the hectic cause by amputation; the pulse falls and grows firmer, diarrhœa and sweating cease, the hectic flush leave the cheek; in short, the constitution makes a complete and successful rally. It is had recourse to in order to take away disease in the following situations,—in the cancellated articulating extremity of a long bone, in part or the whole of a short bone, and in part or the whole of long bones. Even a long bone, from one articulating surface to the other, may be removed; the metacarpal bone of the thumb, and the metatarsal bone supporting the great toe, may, for example, be taken away in their whole extent. I have seen these bones so treated, but the result was unsatisfactory. As has already been observed, the part of the member that is left is without support, and not under the influence of muscle; it is consequently loose and useless.
Operation for the removal of necrosed, or softened and ulcerated portions of the carpal and tarsal bones, is sometimes successful. But operative interference, either with these, or with more extensive and formidable articulations, is not advisable unless the soft parts are not largely involved, and when the general health is tolerably good—the patient either having suffered less than usual, or having rallied and begun to gain strength after exhaustion by discharge and fever. If the ligaments, bursæ, and cellular tissue are much affected, as is often the case, there is no chance of discharge ceasing, and the patient regaining health, even though the bone be removed to any extent—a second operation will be required, namely, amputation above the diseased parts. And when this becomes requisite, after failure of the first to restore or even improve the health, the patient is apt, as has too often been the case, to sink under the accumulation of suffering. He might, even though much exhausted, have been able to bear up against the shock of one and a successful operation, but he cannot endure that of a second, or perhaps third, serious and protracted attack of the knivesman. The disappointed hope of a cure from the first operation is a secondary, though nevertheless a sure contributor towards the unfortunate issue.
No particular rules can be laid down for the operative procedure. By converting two or more natural openings into one, extending the incisions as much as possible in the direction of the limb and of the muscles and tendons, and avoiding the course of the larger bloodvessels and nerves, room is made for an accurate examination of the diseased parts. A strong and firmly pointed knife is required for these incisions, for the soft parts are much consolidated, and are cut with difficulty. The extent of disease is ascertained both by the probe and by the finger, and farther measures, if necessary, are then adopted for complete removal. Loose portions of bone are taken away; and often large sequestra of the cancellated tissue are found lying in the cavity, either loose or easily separable; for extraction, forceps and the fingers, and sometimes a lever, are required. A firm scoop is useful for removing such portions of diseased cancellated tissue as are still continuous with the shaft of the bone. When an opening in the cancellated tissue, leading to an internal sequestrum, is minute, enlargement is effected by means of either the trephine or the cutting pliers: afterwards, gouges, gravers, &c., may sometimes be useful in operating on the soft texture underneath,—but they are seldom requisite. The bleeding from the soft parts is free; the vessels do not retract, and may require the application of a needle and ligature. That from the bone is easily arrested by pressure: the cavity is filled with charpie or with dossils of lint, and these are supported by a bandage. Some days after, this dressing is removed, having been previously softened and loosened by fomentation and poultice. The cavity should now be examined carefully, to ascertain whether or not all the diseased parts have been taken away; it is then dressed daily from the bottom. If parts of the surface assume an unhealthy aspect, the granulations being either backward or flabby, to these escharotics should be applied—the most suitable is the red oxide of mercury. Gradually the cavity fills up, and a depressed, firm, and permanent cicatrix is obtained. It need not excite surprise, however, if, in not a few cases, after matters have proceeded apparently very favourably for some time, the surface become pale, soft, and glistening; the discharge thin, acrid, and profuse; the integuments around tumid and discoloured,—if, in short, the disease be in no long time fully reëstablished.
The tarsal and carpal bones are often the subjects of this operation. In a few cases I have removed several, in others one or a portion of one, with success. In one instance the greater part of the astragalus was taken away, along with the ends of the tibia and fibula. There remained, in consequence, a large opening across the joint, through which a cord was passed, to facilitate gradual and piecemeal discharge of remaining portions of diseased bone. The articulation could actually be seen through. The seton was gradually diminished and the aperture closed. The foot was thus preserved, and the leg was but little shortened; the limb proved strong and extremely useful, but the ankle-joint retained little or no power of motion. I have also again and again trephined the os calcis, and removed large portions of it; the cuboid likewise has been taken away, along with the base of the metatarsal bone or bones in connection with it; in some of these cases an excellent cure followed, in others amputation of the foot was afterwards necessary.
Some have ventured to cut away the articulating ends of the bones composing the knee-joint. This may be accomplished without much difficulty. The patella is either removed entirely or turned to a side, the ligamentous and tendinous attachments are divided, and the ends of the bones thus exposed; by cutting close to and towards them, little risk is incurred of wounding the bloodvessels and nerves in the popliteal space. The saw is readily applied in a horizontal direction. After tying the vessels, and approximating the edges of the wound, the limb is placed in the straight position, and retained fixedly so by the application of splints. Much constitutional disturbance is to be expected, as well as profuse and tedious suppuration. There are few surgeons so rash as to have recourse to this operation. One or two patients, it is true, have lived in spite of it, retaining the limb in a tolerably useful state. But in others,—and these constitute the majority,—amputation was after all required, and that proved insufficient to save the patient. In short, the results of excision of the knee-joint do not justify its repetition.
The articulating ends of the bones composing the shoulder-joint have been removed; and this may be done with advantage on account either of disease or of injury. This joint is, like others, liable to ulceration of the cartilages, either primary, or in consequence of abscess and degeneration of the soft parts around. The disease is attended usually with painful feelings increased by motion, and the patient is indisposed to attempt motion. Sometimes merely weakness of the limb is complained of, and the attention is drawn to the wasted appearance of the muscles, particularly of the upper arm; the deltoid seems shrunk almost to nothing. The motions above the shoulder are lost; and abduction is impracticable. Much pain is produced by pushing sharply the articulating surfaces into contact, and is further increased by rotation. The enforcement of strict and absolute rest of the joint, the establishment of a drain in the soft parts immediately neighbouring, and attention to the general health, often prove sufficient to arrest the progress of this disease. If, however, it is neglected, abscess forms sooner or later. On cutting into this, and introducing the finger, the joint is discovered to be open; the head of the bone is found detached from the soft parts, and unsupported. Or this state of parts may be ascertained to exist by examination through a sinus, either with a probe, or with the finger after dilatation. In these circumstances, an attempt may be made to check disease, and preserve the arm, by excision of the obnoxious parts of the bone. And this kind of operation is also justifiable when the head of the humerus has been shattered by musket-shot; or when it has been exposed and injured by a splinter, or by a large shot, and the joint laid open. The situation and course of the incisions will be so far regulated by the openings or wounds already existing. They should always be made in the direction of the fibres of the deltoid, and the posterior aspect of the articulation is preferable to the anterior. One incision, from the back of the acromion process to near the insertion of the muscle, is sufficient to expose the head of the bone, to allow all its remaining attachments to be separated, and to admit of its being turned out so as to be conveniently acted on by the saw. The head of the bone merely is taken away. In separating the soft parts from its neck, the edge of the knife should be always directed to the bone, to avoid the nerves and vessels on the inside. In some cases of injury, very little additional wound may be requisite. The glenoid cavity may, in consequence of being seriously involved in disease, also require removal; this is best accomplished by large cross-cutting pliers. Few vessels require ligature. The edges of the wound are brought together; the elbow is supported, and the arm fixed to the trunk, in order to keep the bones in apposition, and prevent motion. This position must be retained during the rest of the cure; and when the wound is on the outside of the shoulder, as recommended, the dressing of it does not interfere with the retentive apparatus. The discharge gradually ceases, and cicatrisation is obtained, though not till after a considerable time, at least in general. The cut ends of the bones accommodate themselves to each other, and a sort of new joint is formed—but never strong. The motions of the forearm are perfect, though perhaps weakened; those of the upper arm are very incomplete. I have both performed and assisted in the operation repeatedly, and never experienced any difficulty; a cure has not always followed, but in some cases the limb has become very useful.
The elbow-joint, on account of its exposed condition, is generally regarded as the most favourable for excision. The affections of the joints of the upper extremity are much more manageable than those of the lower, and may generally be prevented from proceeding so far as to end in destruction of the apparatus. By care and good management, disease will be arrested, and the functions and motions of the parts restored and preserved; or the articulation may become stiff, and even though the anchylosis be complete, the limb will be very useful if the joint have been kept in a good position. The health, if previously undermined, is renovated, so soon as the local disease is arrested. But some bad cases are met with, in which all the parts surrounding the articulation are involved, and the strength wasted; in these amputation is the only safe and effectual procedure. It is only when the soft parts are not much diseased, when it is ascertainable that the affection of the bone is only to a limited extent, and when the usual means of cure have had a fair trial and failed, that excision is admissible. In determining on the operation, the time of life and the worldly circumstances of the patient are to be considered: a poor man requires his limb to be serviceable in labour; handsome appearance without utility is to him of no value. The motion and usefulness of the arm may be in a great measure preserved, if only a part of the bone of the arm, or a part of those of the forearm, entering into the articulation, be removed; but if large portions of all of these be taken away, the muscles will lose their support, the motions will never be restored to any extent, and the motion that is of it will be weak and vacillating. The joint will remain loose and powerless, and the limb will prove to be but a useless incumbrance. Such, at least, is the result of my experience on this subject; and I am sorry to add, that all which has been written on it is not deserving of unreserved belief. Many patients have, after long and severe suffering, preserved the arm to little purpose; others have been necessitated to submit to another operation—amputation after all; some have died after the first, others after the second mutilation. The operation is attended with no difficulty in execution, and this in some measure accounts for its frequent, and it is to be suspected, indiscriminate, performance of late years. The incisions are made on the posterior aspect of the joint. One is placed in the mesial line, extending from about two inches above the olecranon to the same distance below it; and from this flaps are raised, by making either a cross-cut in the middle, or one at each extremity; in the one case the flaps are four, and triangular; in the other two, and quadrangular; by either method the bones are readily exposed. A more simple form of incision, as described in the Practical Surgery, will often be found to suffice. The joint is opened and dislocated, and the soft parts separated to the necessary extent from the bones. The ulnar nerve is avoided by dissecting close to the bone. The diseased portions are then sawn off. The wound is closed, and the arm kept bent. This operation I have performed pretty often, the cases being carefully chosen for it, and the success has been highly satisfactory. By the sanguine supporters of this operation, the after-treatment is advised to be conducted so as to secure motion in the new articulation. From this I would dissent, for if the articulating ends of the bones have been actually cut off, the motion may be extensive enough certainly, but both joint and limb will be almost altogether impotent. It would be better to procure anchylosis in the bent position, than to have the arm dangling like a flail; in the one case the limb will be useful; in the other, ornament, and that too of an equivocal kind, is all that it can boast. Even anchylosis, in most cases, can be brought about only after the lapse of a long period. In the more severe affections of this joint, amputation of the limb is the operation which must ultimately be had recourse to, if the patient survive; and it is better to perform this at once, than after the experiment of excision has been tried and found wanting. I know that parents have too often had to regret and mourn bitterly their having departed from sound advice, and lent themselves to such experimental trials on their offspring.