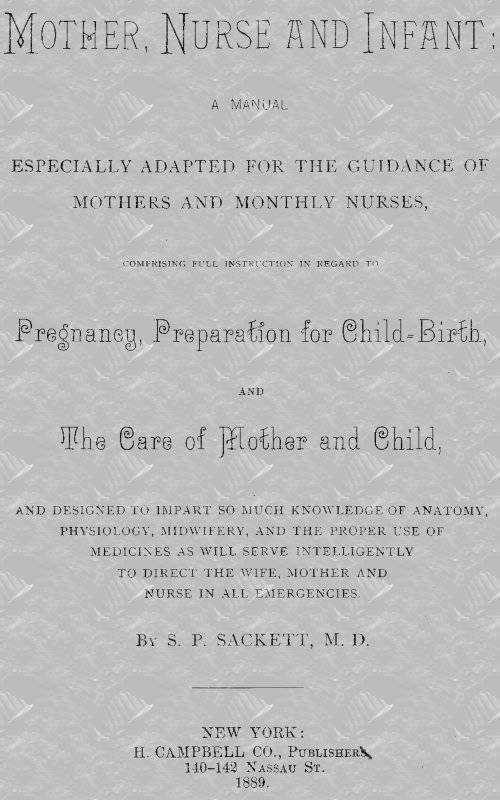
Fig. 14. Retroflexion of the uterus.
The condition known as retroflexion consists of a bending back of the uterus at a point where the neck joins the body, so that the fundus is found between the cervix and rectum, the os uteri being in the natural position.
In antiflexion we find the fundus pressing upon the bladder. These displacements are rare in virgins. The false membrane formed in peritonitis is now and then the cause of these deviations, when there is superadded such causes as are mentioned for prolapsis. The symptoms of RETROFLEXION are usually a dull, weary and constant backache, which is more marked about the sacral region, pains that shoot down the thighs or the groins, and a frequent desire to go to stool, although nothing comes away. The passage of a motion that is not at all constipated aggravates the pain and aching; sexual intercourse is attended with suffering, and is not followed by pregnancy; and just before and after the monthly periods there is so much tenderness that sexual connection cannot be tolerated.
Fig. 15. Antiflexion of the uterus.
The catamenia come on with pain and difficulty, but about the second day the flow of blood seems to give some relief. The general health is bad, there are frequent attacks of nausea, the appetite is small, the spirits are depressed, and there are many what are called hysterical symptoms. On examination the congested fundus may be found encroaching upon the rectum; on touching this part the patient will exclaim that it is the seat of her sufferings, and it is not uncommon to find tenderness of one or both ovaries.
Not many of these symptoms are present in ANTIFLEXION, but this commonly produces great irritability of the bladder, so that when the patient is in the erect position, the desire to micturate is almost as great as in disease of the bladder.
Fig. 16. Anteversion of the uterus.
The treatment includes replacing the uterus with the sound. Should there be adhesions, however, this might cause intolerable pain. In such cases relief is given by the use of belladonna plasters and belladonna, opium, hyoscyamus, or conium tampons. One-half to one dram of the tincture of one of the narcotics may be added to the glycerine in which the tampon is soaked, or the cervical end of the tampon may be dipped in the tincture. Suppositories and ointments may also be used. (F. 163, 214).
RETROVERSION AND ANTEVERSION.
In RETROVERSION (Fig. 13) the fundus is turned toward the hollow of the sacrum, while the os is drawn under the arch of the pubis.
Anteversion is characterized by the fundus being towards or against the bladder, the os being directed to the cavity of the sacrum. (Fig. 16.) Retroversion is liable to occur at the third month of pregnancy, from the neglected distention of the bladder, and from a morbid weight and enlargement, though after the fourth month the uterus is too much enlarged to fall down in any way. The chief symptoms are backache and bearing down pains. It may happen that micturation will be impeded; and if the bladder may be felt at the lower part of the abdomen, or if the patient complain of a constant desire to pass water, or especially if the urine should dribble away, the catheter ought to be passed without loss of time, and the bladder should be kept evacuated. It may be necessary, in order to restore the organ to its proper position, to introduce the first and second fingers of one hand into the vagina, and a finger of the other into the rectum.
CHAPTER V.
Mismenstruation.
AMENORRHŒA.
The first variety of cases of amenorrhœa are those where no menstrual fluid has ever been secreted. All girls, as we have seen, do not menstruate at fifteen years, as all children do not cut their first teeth at seven months, and in either case there may be no disease. But when a female has reached adult life, when her frame has assumed the character of womanhood, when she is not chlorotic, and when all her organs (save the sexual) perform their functions naturally, then a cause of the absence of the flux should be looked for. Menstruation may be absent from congenital malformation. The ovaries may be wanting, or if present may be atrophied or diseased; perhaps they present scarcely a trace of a Graafian vesicle; or these glands can exist and the uterus be absent or imperfect; or there may not be found a trace of a vagina. In the second variety of amenorrhœa there has been a secretion of the menses but no evacuation of them. This may be because there is an occlusion of the vagina, or the os uteri may be imperforate. When the os is closed by a membrane, the structure may be incised with the bistoury, or perhaps be ruptured by the uterine sound.
The third variety is the most common form of amenorrhœa, viz: that in which the flux having been properly established and appearing regularly for a time, has been prematurely arrested. But it may be said of amenorrhœa in its various forms, that it is not so much a disease as a symptom of disease; a consequence of either individual organization, disorder of the uterus or ovaries, or of some other organ or organs sufficiently important to affect the constitution.
Hence all the means that restore the system to health, medicinal and hygienic, may be recommended as tending to cure the complaint, and hence we have to inquire whether there is serious disease in any of the organs when the question of pregnancy arises, on account of the disappearance of the menses.
It is always necessary in treating amenorrhœa to consider the cause of it, and we should know that it may come from torpitude of the secernent vessels of the uterus, produced by anxiety of mind, cold, or suddenly suppressed perspiration; falls, especially when accompanied with terror; or a general inertness and flaccidity of the system, and more particularly of the ovaries. (F. 172, 173).
DYSMENORRHŒA.
There are few women who pass through the whole period of sexual vigor without having more or less frequently to endure an attack of dysmenorrhœa. Some few females experience great pain with each flow, from puberty to the change of life, while in others pain is only an exceptional accompaniment. With some women marriage effects a cure, while in others it either aggravates or originates dysmenorrhœa. Three distinct varieties of dysmenorrhœa have to be considered: the neuralgic, the congestive, and the mechanical.
The variety which is called NEURALGIC DYSMENORRHŒA is more frequent in unmarried females; and if married, in those that have not borne children; and most frequently affects those of a nervous temperament, and of a thin, delicate habit. The paroxysms present all the characteristics of neuralgia. For a time before the catamenia appear there is a sense of general uneasiness, a deep-seated feeling of cold and headache, sometimes alternating with pain in the back and lower part of the abdomen, perhaps extending down the thighs.
The flux comes on sometimes slowly and scantily, or in some cases in slight gushes. The discharge may be paler than natural, and may be mixed with slight clots. In some cases there is a membrane of plastic lymph discharged either in shreds, or in the form of the uterine cavity that it has lined. Conception is rare under such circumstances.
Though the disease seems to be of a simple neuralgic character, it is supposed that there is a degree of inflammation of a peculiar kind in the mucous membrane where the plastic lymph is thrown off.
In regard to the duration of the period, the constitutional injury sustained, and as to the relief on the appearance of the menses, the cases vary.
A peculiar irritability of the uterus is a common cause of this form of the disease, but, like amenorrhœa, it may be caused by cold, mental emotion, or local injury from a fall.
In the treatment of this class of cases, to reduce the pain, opium, conium, hyoscyamus, etc., are given, often combined with camphor. (F. 161, 163, 166, 167.) These should be given in the form of an enema, or a suppository, if the stomach is irritable. (F. 160.) The hot hip bath should be employed, the patient remaining in it from thirty-five to forty minutes; an ounce of carbonate of soda may be added to the water. The good effects of the bath may be kept up by the use, immediately afterwards, of a pessary of oxide of zinc and belladonna. (F. 163.) It will be of benefit to take vaginal injections of tepid, or warm, or hot water on the approach of the menses, and the patient should use a pediluvium, or a hip bath, for two or three nights in succession antecedent to the show of the menses. During the interval every effort should be made to strengthen the patient, and to diminish the irritability. Injections of tepid or cold water may be taken daily; the diet should be nourishing, and plenty of exercise in the open air should be taken by the patient. Some preparation of iron should be given, and I have found F. 177 particularly useful.
Congestive dysmenorrhœa, sometimes described as inflammatory dysmenorrhœa, generally comes on at a later time of life than the neuralgic form. It occurs in females of a full habit and of a sanguine temperament; in the married as well as the unmarried, and those that have not borne children.
Restlessness and feverishness, rigors, flushing and headache generally precede the severer symptoms. The sufferings commence, or are generally aggravated four or five days before the period, and it may continue for a week or more. Both before and after the catamenia appear, there is great pain across the back, aching of the limbs, intolerance of light and sound, weariness, the face is flushed, the skin hot, the pulse full and bounding; when the flow gets abundant the pain is mitigated, though there are paroxysms of pain, as small clots and shreds of membrane are thrown off from the uterine cavity. Under the influence of inflammation, the epithelial coat of the uterine cavity and of the vagina is sometimes expelled. In the interim between the periods the cervix uteri is congested and tender, and pain will be excited by pressing the ovaries; usually there is a tenacious leucorrhœal discharge. Frequently the breasts swell and become tender as the period approaches.
In treating this form of dysmenorrhœa, opiates must be used, as in the former variety, to afford some alleviation. Give also saline purgatives, febrifuge medicines, such as aconite, veratrium, and gelsemium; also cooling drinks. During the interval the patient should live plainly, avoid stimulants, and take moderate outdoor exercise. The suppositories (F. 163) may be used steadily. If the disease be associated with a rheumatic diathesis, the appropriate remedy for that should be used. It is in such cases especially that chalybeate mineral water, warm sea water, baths, colchicum, iodide of potassium, with friction and electricity applied directly to the hypogastric region, succeed in restoring health. (F. 103, 165).
Mechanical dysmenorrhœa is that form in which there is some mechanical obstruction to the escape of the menstrual discharge. The causes of the obstruction are various. There may be either a stricture of the internal orifice of the uterus, or a narrowing of the whole canal of the cervix, or the external os uteri may be small and contracted, or some tumor may interfere with the patency of the cervical canal, and there may be retroflexion or antiflexion of the uterus.
In these cases there is more or less violent expulsive pain coming on in paroxysms, and there is usually a scanty flow. Often the discharge escapes in gushes, each gush being preceded by a bearing down effort, and accompanied by an expulsive pain. There are attacks of nausea, restlessness and retching, with flatulence; there is always severe headache and congestion, with tenderness of the ovaries; and if there is endometritis, there are some other inflammatory symptoms.
Modern gynecology has various remedies for this class of cases, of which it is not necessary to speak here.
MENORRHAGIA.
The term menorrhagia should be applied only to cases of menstrual flow, although it is often employed to signify any considerable sanguineous discharge from the uterus, other than normal monthly escape. But I will say something here of cases where there is a more abundant or a more prolonged flow than is natural to the subject of it, and of cases where there is a recurrence of the discharge at short intervals, so as to seem almost continuous.
In that variety in which the discharge is normal in quality but the quantity is increased, there is undue uterine congestion, set up by constitutional causes, or it is induced by slight disease of the uterus or ovaries.
When menorrhagia takes place in plethoric habits, it is manifestly remedial, and ought not to be restrained hastily. We may endeavor to reduce the plethora, and a cooling diet, the recumbent position, and saline cathartics may be enjoined. (F. 61).
If the flow continues five days or more, and especially if depressing effects are manifested, such as general weakness, languor, mental depression, with pain in the head, loins or back, the patient is undoubtedly suffering from the loss of blood, and it is best to restrain the flux by general and local means (F. 176.) At the time when the flow is profuse or long continued, give strong cinnamon tea, a teacupful at a time, or teaspoonful doses of tincture cinnamon every hour. Astringent pessaries should sometimes be used. Formerly injections of cold water were given; recently injections of hot water, as hot as can be borne in the vagina, are considered more effectual. Fluid extract of ergot, in half-teaspoonful doses, may be given every hour for two or three successive hours. Other remedies are elixir vitriol and turpentine, opium and acetate of lead during the attack; and counter irritation to the sacrum, the douche to the loins, sponging, cold vaginal injections, and the sitz bath during the interval. (F. 175).
If astringent or cold injections are used, the patient should lie upon her back in bed, and the fluid should be thrown up gradually. Of course, there are cases where only an experienced, well-educated physician can do all that is required in removing the cause of the difficulty.
CHAPTER VI.
GENERATION.
Generation is effected in the human species through the medium of the two sexes; to effect it there must be the actual contact of the male semen, or its spermatozoa, with a healthy Graafian vesicle.
In CONCEPTION the SPERMATIC FLUID is furnished by the male. When this is examined under the microscope it exhibits a great number of little bodies, which are moving; these are termed spermatic animalcules, or spermatozoa. These are met with in all animals capable of reproduction, and they do not appear in the human species before puberty.
The ovule furnished by the female is existent in the ovary at the marriageable period. Fecundation takes place in the ovary; probably, sometimes, also in the tube or uterus when the ovule is passing out after menstruation.
Ordinarily the fluid ejaculated by the male must reach the uterus, and in some way be conveyed to the ovaries through the Fallopian tubes to produce fecundation.
It is believed that, as the consequence of copulation, the semen is thrown on the neck of the uterus; that it is carried forward, first, by the movements proper to the uterus and tubes; second, by the movements proper to the spermatozoa till it reaches the ovum, generally in the ovary; that it enters the ovum, and that then fecundation takes place.
Upon being impregnated and the vesicle bursting, the ovum is grasped by the free extremity of the Fallopian tubes, which is in contact with the ovary, the ovum passes from the ovary to the canal, is pressed onwards by the peristaltic motions of the tube through the duct, and finally reaches the uterine cavity; there it continues to grow during the ordinary term of gestation. After two hundred and seventy days the ovule has developed into a child, and is expelled through the natural parts of generation. When gestation proceeds in this manner, it is said to be normal, or good, or uterine; sometimes (though very seldom) the ovule is arrested at some point in its passage, and is developed outside of the womb; this is termed an extra uterine pregnancy.
The time at which conception is most likely to occur is that immediately following the flow of the menses; it may take place immediately before the flow, and sexual intercourse may be fruitful even when it takes place in the middle of the interval between the sexual periods, though the latter is unusual.
When conception takes place a few days or a few hours before the period, it is not followed by the menstrual flow.
UTERO-GESTATION.
At each menstrual period the bulk or size of the uterus is for the time increased, and if conception takes place about that time, the excitement maintains and soon increases the enlargement. The mucous membrane becomes almost doubled in thickness, and when the ovule arrives in the womb, it finds it filled with the membrane, the whole uterus is congested, its vessels enlarge, and are filled with blood, many which were invisible before are now filled with red blood, and the whole form an intricate network on the surface, and in the substance of the organ; the coats of the arteries increase in thickness; the coats of veins are thinner, and admit of still greater distention; the nerves increase in size, and may be seen accompanying the blood-vessels, and there are changes not only in the volume, but in the shape, situation, direction, and relations of the uterus.
The organ increases slowly in size during the early. months of pregnancy, and more rapidly in the later. The walls are distended, however, not mechanically from the development of the ovum, but simultaneously with it, and from a physiological cause; in shape it becomes rounder, and towards the end of pregnancy it has an ovoid form. Simultaneously there is an alteration in its position; at first the neck subsides towards the floor of the pelvis; the presence of the rectum may incline the fundus to the right and the neck to the left; about the fourth month the uterus rises above the superior strait; at four months the fundus uteri is two or three fingers in breadth above the pubis; at five months it is within one finger’s breadth of the umbilicus; between the fifth and sixth month it passes the umbilicus; at seven months it is three fingers’ breadth above the naval; at eight months it is four or five above, but it does not rise higher during the last month. While it is rising it follows the direction of the axis of the superior strait; afterwards it inclines to the right oftener than to the left.
At term, the superior part of the uterus is in contact with the abdominal walls usually, but sometimes there may be some of the intestines interposed between them.
At full term the parietes of the womb are thicker than in the unimpregnated condition; at the point corresponding to the insertion of the placenta, thinner at the neck, and otherwise it retains about its original thickness.
The uterus increases about forty times in weight during pregnancy; at term it weighs about twenty-four ounces, and its length is from twelve to fourteen inches, its breadth from nine to ten, and its depth, antero-posteriorly, eight to nine inches.
The os uteri, after it is in the gravid state, becomes somewhat swollen, but soft and cushion-like. This softening is at first superficial. Towards the end of the third month, the lips of the os tincæ are softened throughout their whole thickness, and the softening increases from below upward.
The neck of the uterus seems somewhat elongated at the first, but at the commencement of the sixth month the length of the cervix seems to diminish; there is, however, no considerable shortening until the middle of the eighth month; during the last fortnight of pregnancy it diminishes very rapidly, and finally is totally effaced.
In primapara the os tincæ is rounded at first, and is not dilated. In females that have had children the external orifice is widely open, and the cavity in the neck is funnel-shaped, continuing to increase until it reaches the internal orifice.
As gestation progresses the texture of the uterus changes. The peritoneum spreads out in all directions without a decrease in thickness; the mucous coat becomes apparent, it grows redder and more vascular, and its folds disappear; the glands of the body of the womb grow longer; the middle coat is enlarged by the increase in size of always existing muscular elements, and the formation of new fibres and increased connective tissue. There is, towards the end of pregnancy, an astonishing development of the vascular system; the lymphatic vessels acquire considerable calibre, and the nerves are developed in every way, although the neurilemma is most affected.
The changes developed in the uterine mucous membrane are of especial interest. Its vascularity is greatly increased during menstruation, the glands are enlarged, the membrane thickened, thrown into folds and becomes of a violet color; this condition continuing until the ovule is discharged, or until the last of the menstrual period. The fecundation of the ovum will maintain and increase this vascular condition of the membrane. Its vessels are so enlarged as to cause small effusions beneath the epithelium, which gives to the internal surface a spotted appearance; after two or three weeks it is still more mottled, more puffed up, and furrowed with folds and wrinkles. This membrane is the decidua, which is afterwards expelled, with other contents of the uterine cavity.
The DECIDUA REFLEXA is a fold of the decidua in which the fœtus is enveloped, and both of these membranes, which are at the last expelled with the fœtus, are developed from the uterine mucous membrane. The uterine decidua, after the second month, grows thinner, and its folds are gradually effaced; after the fifth month it is only one twenty-fifth of an inch in thickness, and it is still thinner at the termination of pregnancy. At the fifth month it is separable from the uterus, and the first trace of the new membrane which is to replace the decidua may be detected under it. A partly uterine membrane may be thrown off when an abortion occurs, during the early months of pregnancy.
CHAPTER VII.
THE OVUM AND ITS DEVELOPMENT.
The ovum at maturity (and not impregnated) is described as being composed of the vitelline membrane, which seems like albumen in appearance, but is a thick, transparent membrane, without determinate texture; second of the vitellus or yolk, a granular liquid contained in the vitelline membrane, composed of a coherent transparent viscid mass; third of the germinal vesicle, which is composed of a transparent colorless membrane, enclosing a liquid also transparent; and lastly, of the germinal spot, that is held in suspension in the liquid that the germinal vesicle contains.
The ovum passes slowly through the Fallopian tubes, and during the twelve days or more that it is passing to the uterus, there is some development, some increase in size, and by the time it has reached the uterus it has become impossible to find in it either vesicle or germinal spot.
It is probable that in its passage it is nourished by the granulations which accompany it, and by absorbing the liquid secreted by the oviduct.
As the impregnated ovum is developed, the chorion, the amnion and the embryo may be observed.
The chorion, which corresponds to the membrane lining in the shell of an egg, is found covering the ovum at the earliest period that it has been seen in the uterus. It is smooth internally, but externally it is covered with short round villi, which at a later period remain only where the placenta is developed. The chorion is enveloped in a great measure by the reflected decidua; there is at the outset considerable space between the two, mostly filled at first by the villi of the chorion, though there may be between the two an effusion of blood; these villi soon disappear, and the membranes come in contact.
In that part of the chorion that is not covered by the decidua reflexa, the villi are more and more developed, and they contribute a most important part in the formation of the placenta.
At the same time that the placenta is formed, the villi on the other portion of the chorion is obliterated, so that the principal part of the chorion is a thin, colorless, transparent membrane, united outwardly to the reflexed decidua by short, delicate filaments, and inwardly to the amnion by an albuminous layer called the tunica media.
There is also between the two membranes the vesicula alba. This bears a perfect analogy to the yolk of an egg; it is the vitellus surrounded by the blastoderm. Its use is to contain nutriment for the fœtus before the development of the placenta.
The amnion is the most internal membrane of the ovum; it is continuous with the margins of the ventral opening in the fœtus, and closely envelopes the embryo in the early period. Its internal surface exhales a liquid into its own internal cavity, and in this the embryo swims freely.
As this membrane is more and more filled, it presses back the exterior liquid and thereby condenses it until the amnion comes in contact with the chorion. And since it adheres to the abdominal parietes of the fœtus, it furnishes as it extends a membranous sheath to the allantoid and umbilical vesicle, and these vessels, and all parts thus enclosed constitute the umbilical cord.
The placenta is an appendage of the chorion; it is a soft, spongy mass, constituting the principal connection between the ovum and the uterus, being destined to the hematosis and (as we suppose) to the nourishment of the fœtus. The placenta, at the termination of utero gestation, is a flattened body about an inch in thickness at the center; its shape is circular or oval, and it is from six to eight and one-half inches in diameter; its internal surface is covered by the chorion and amnion, and exhibits plainly the umbilical arteries and veins which converge to form the umbilical cord. Its fœtal portion is formed by the hypertrophied villi of the chorion, with which its circumference is continuous, and its maternal portion is continuous with the decidua, and is in fact a thickened part of that membrane. As the villi of the chorion are developed on one part of its surface, they ramify and form filaments that engraft themselves upon the uterine mucous membrane and adhere closely. At the same time there is an inverse development of the uterine vessels, which form vast numbers of loops that descend between the villi of the chorion, and extend through to the fœtal surface of the placenta. An amorphous matter is soon thrown out which unites the two parts together.
The placenta is, therefore, composed of two parts, distinct in their physiological action, though they together present but one mass to our view. One part is the fœtal portion formed from the chorion; the other is the maternal portion formed from the uterine mucous membrane, of which it is a greatly thickened part. After delivery the fœtal placenta comes entirely away with the epithelial layer of the placental decidua, and the placental distribution of the maternal vessels; a portion of the maternal vessels remains attached to the uterus.
The placenta may be inserted upon any part of the uterine cavity, although it is most usually near the fundus where the ovum must enter the womb. If, as is sometimes the case, it is attached at the lower part, over the orifice of the womb, it causes unavoidable hemorrhage in the later months of pregnancy.
The umbilical cord, funis, or naval string, is the connecting link between the child and mother. It commences when the external lamina of the blastoderm with the alantois are so changed as to form a mere cord upon which the two umbilical arteries ramify, and when all these have an enveloping sheath from the amnios. It may be discerned in this state at the end of the first month; at that time the fœtal intestines may be seen to protrude beyond the umbilicus into the amnionic sheath, but the cord is then cylindrical and very small. There are progressive changes, the cord becomes simplified, the canal of the amnionic sheath is obliterated gradually at its extremity, and as the effacement proceeds towards the umbilicus the intestine is pressed back so that no hernia remains.
There are two arteries in the cord; these arise from the abdominal aorta in the fœtus; they go by a flexed and tortuous course to the placenta, where they ramify and are distributed. There is only one vein which returns the blood from the placenta; there the radicles coalesce to form the branches; these unite to form the umbilical vein. This is not as flexuous as the arteries, which, being longer, wind around the one venous trunk. After the third month these may be plainly seen in the sheath imbedded in what has been called Wharton’s gellatine.
Ordinarily the cord lies free and loose in the cavity of the amnion, but occasionally owing to the movements of the child it may be coiled around the child’s neck, be tied in knots, or it may escape below the head so as to prolapse during labor.
The length of the cord varies; it is very rarely less than eight inches, and it is sometimes six or eight feet long.
After the birth of the child, the pulsation in the cord ceases within about fifteen minutes. After the cord is cut that portion that is attached to the umbilicus dies and usually falls off about the fifth day.
The blood of the fœtus is ærated or undergoes a change in the placenta analagous to the change that our blood undergoes in the lungs.
CHAPTER VIII.
THE FŒTUS.
The embryo first begins to be distinct about the third week; is then about two lines long, weighing one to two grains; is surrounded by an amnion which lies loosely about it, and obviously proceeds from the abdominal laminæ; it presents cerebral vesicles; there is the appearance of an eye, several arteries are seen though not distinctly formed; the abdominal cavity is open for a considerable extent in front.
About the fifth week the embryo becomes more consistent; the head is disproportionately large; rudimentary eyes are indicated by two black spots; the abdomen is nearly closed, though at the umbilical aperture a loop of intestine escapes; the abdominal members are present, and the cord exists in a rudimentary condition; the embryo is nearly two-thirds of an inch long and weighs about fifteen grains.
The successive changes in the development were, 1st, a germ membrane visible immediately after the bursting of the vesicle; 2d, at some point an aggregation of granules forming the cumulus of the blastoderma; 3d, the embryo developed lying at this point, as it were upon the membranes, which consist of three superimposed laminæ or layers; 4th, on the serous layer arise the organs of animal life, the brain and spinal marrow, organs of sense, skin, muscles, tendons, ligaments, cartilage, and bone; on the mucous the organs of vegetative life, the intestinal canal, lungs, liver, spleen, pancreas and other glands. The heart and vascular system arise from the vascular layer (if this can be considered a separate one).
About the second week, or perhaps the third, there is a mass of globules loosely connected together forming the primitive streak of Von Baer, and around this the area vasculosa is developed. The globules of the primitive streak, seem next to be developed into two laminæ dorsales, which is the axis of the future embryo, and the origin of the spinal column. That portion of the fluid that separates the chorda dorsalis from the lamina dorsalis is the future spinal cord, and brain. Two other lamina—laminæ ventrales of Von Baer—are in the mean time proceeding from the axis of the embryo, one on each side; they grow laterally and converge below the axis.
After the rudiments of organic life have been commenced in the central portion of the serous layer, a fold of its peripheral portion arches over the dorsal surface of the embryo so as to represent a sac, and is composed of two membranes; the one next to the fœtus is the amnion, the other is gradually separated from the amnion and joins the serous lamina of the blastoderma; this is the false amnion of Pander.
The heart is formed at this early period, and although there is no septum between the ventricles, a vein may be seen entering into it, and an artery passes out which divides into four branches to be distributed and ramified in different portions of the fœtus.
The abdomen is yet an open cleft, in which (but projecting beyond it) is the heart, which is of very large dimensions; behind the heart is the liver, and under the liver the intestine which is attached by means of a distinct mesentery. At this period (three weeks) the lungs are constituted of five or six lobules, and two large glandular structures may also be discerned along the vertebral column, which are called Wolfian bodies; these anticipate the function of the kidneys. The alantois is seen arising from the lower part of the intestinal canal on a little vesicle and extending so as to encircle the embryo.
During the second month the extremities are growing, and become more projecting; the body is curved and the head bent downwards; there are indications of the nostrils and a gaping oral aperture; the forehead is more swelled because of the development of the hemispheres of the brain; the spinal cord is cylindrical of nearly uniform thickness and terminating in a blunt extremity—posteriorly it is open; the medulla oblongata makes a bend forwards at the top of the neck, and then ascends perpendicularly into the capacious cranium.
The first centres of ossification appear about the seventh week on the clavicle and lower jaw. At this time the kidneys and renal capsules begin to appear. The only trace of muscular fibre is in the diaphragm. The vertebral arches are not yet closed in, and the ribs appear like little streaks; the liver is very large and granular. The stomach is assuming somewhat of its normal form; the urinary bladder is enclosed, but the anus is imperforate. At this time the embryo is about an inch in length.
At two months the rudimentary organs of generation may be distinguished, but their development does not clearly show the sex. The embryo is from one and a half to two inches long and weighs near half an ounce, the head forming two-thirds of the whole.
After this period the different parts are developed with tolerable rapidity. At ten weeks the embryo is about two and a half inches in length. At the end of the third month it is from five to six inches long and weighs from three to four ounces. The thorax is closed at all points but is only slightly developed; the cord contains no intestines, and its spiral turns are evident; the nails are beginning to appear; the sex is distinct, and the skin acquires some consistence. At the fourth month the fœtus is six to eight inches in length, and weighs from seven to eight ounces. A fœtus born at this period might live for an hour or two. At five months the length of the body, including head and feet, is from eight to ten inches, and weighs from eight to eleven ounces; at six months the weight is about one pound, and the length is eleven to twelve and a half inches.
At seven months the fœtus is from twelve and a half to fourteen inches long and weighs from three to five pounds. The hands and feet, including the nails, are developed; all its parts are tolerably firm, and their respective dimensions better proportioned than formerly. The scrotum usually contains one or both testicles, they having descended through the inguinal ring, from their original place near the vertebral column; the eyelids are partly open; the skin is very red and covered with down. Many children live and are reared that are born at seven months.
The length of a fœtus born at term is eighteen or nineteen inches, though the utmost limit is more than two feet. The usual weight is from six to seven pounds; children have been born, however, that were as much as eighteen pounds in weight. I suspect that this will never occur unless the term has been extended beyond the usual period.
At term the fœtus that is twenty inches long will generally measure ten and a half to eleven inches from the crown to the umbilicus. The different parts are well developed and partly covered by a smegma called the vernix caseosa; the head has attained the proper hardness, and the scrotum usually contain the testicles. In female children the nymphæ are generally covered entirely by the labia, the breasts project, and in both sexes contain frequently a milky fluid.
As soon as the child that has been carried the full time is born it usually cries, opens its eyes, and makes some struggling motions with its limbs; it soon passes urine and feces, and readily takes the breast.
With occasional exceptions the position of the child is unaltered from an early period of pregnancy to its termination, whether the head be upwards or downwards. The arms are generally folded over the chest, the knees drawn up to the abdomen; the back curved, and the head bent upon the chest, so as to occupy as little space as possible. In ordinary cases the head is directed downwards, and the face looks obliquely, so that in the first and second position the back of the fœtus is turned partly forwards, and the belly in the third and fourth. We are enabled in many cases to ascertain the position of the fœtus in the uterus before labor has commenced, by means of the stethescope, by noting whether the pulsation is felt on one side or the other of the abdomen and observing whether it is heard clearly or not.
The longitudinal diameter of the head is from 4 to 4½ inches, the transverse from 3½ to 4, the vertical 3 to 3¾ inches. The transverse diameter of the shoulders and thorax is 4¾ to 5½; the widest diameter of the hips 4 to 5 inches. In general the measurements are a little less in the female than in the male.
The head of the fœtus is large, and as it is less compressible at term than other portions it merits a particular description; we should be acquainted with all its characters, that we may recognize them and thereby determine the position during labor.
The fœtal head is ovoidal in form, the large extremity being posterior. Several bones enter into the formation of the cranium; they are, 1st, the frontal bone forming the forehead; in the fœtus even at term it is usually divided; 2d, the two parietal bones, one on each side of the head, meeting on the median line at the top of the head; they help to form the vault of the cranium; 3d, the occipital bone, forming the posterior and part of the base of the skull; and 4th, the temporal bones, one on the right and one on the left side below the parietal, completing the lateral portions of the cranium and contributing to form the base of it. The cranial bones are not united to each other by sutures as they are in the adult, but are separated, the parietal bones especially, by membranous intervals, the intervals being larger in some children than in others. These intervals, or sutures and fontanelles, must be carefully studied.
The sagittal suture is the antero-posterior one, and extends from the root of the nose to the occipital bone. It is formed in front by the interval that separates the frontal bone into two halves, and superiorly by that between the two parietals. There is a suture which crosses this, called the transverse or coronal suture, which is formed by the space existing between the frontal and parietal bones. When the sagittal suture arrives at the superior angle of the occipital bone, it seems to part and give rise to two oblique lateral sutures which are called lambdoidal; these are formed by the posterior borders of the parietal bones and the superior one of the occipital.
Just at the point where the coronal and the lambdoidal sutures join the sagittal one, two membranous spaces, larger than those just described, are found; these have received the name of fontanelles.
In cases of head presentation during labor, one or the other of the fontanelles may be felt by the attending practitioner, and this indicates to him the position of the head and the presentation.
The anterior fontanelle presents an extensive surface at the place where the transverse crosses the sagittal suture. It is lozenge-shaped, and is bounded by four bony angles.
The posterior fontanelle is formed by the union of the two lambdoidal sutures with the termination of the sagittal suture. It is smaller than the anterior one, and is of a triangular form. It is bounded by the occipital bone and the angles of the parietal bones. During labor the bones may overlap each other so that the sutures cannot be felt, but the prominences of the bony margins will aid the diagnosis.
THE PHYSIOLOGY OF FŒTAL LIFE.
The ovule, after it arrives in the uterine cavity, comes in contact at all points with the mucous membrane of the uterus. Its nutrition at first is organic by superficial imbibition; afterwards, probably the villi of the chorion imbibe the fluids there secreted, and transmit them into the space between the chorion and the amnion, thence it transcends through the walls of the amnion, and a portion is conveyed into the fœtus through the umbilical vesicle. After the placenta is formed there may still be some absorption of some of the nutritive matters contained in the liquor amnii through the skin of the fœtus, but its growth is principally maintained by an assimilation of that which the radicles of the umbilical vessels take up in the placenta. By means of the extensive contact existing between the vascular apparatus of the two placentas, a transudation probably takes place of some part of the maternal blood, which is absorbed and mingled with the fœtal blood, and furnishes some of the nutritive material.
When mingled with the fœtal blood, the nutritive elements supplied by the mother are devoted to the development of the organs. It is supposed, however, that they undergo changes in the large liver of the fœtus and in its intestines.
There is no true respiration in the uterine cavity, but one function of the placenta is to renew the blood of the fœtus from that of the mother, in about the same way that the blood of fishes is ærated by the water passing through the gills.
Whether in the earlier months absorption is carried on by the surface alone, or whether a portion of the liquor amnii finds its way to the stomach is difficult to decide, but, without doubt, a certain amount of digestion is carried on.
The CIRCULATION of the blood in the fœtus cannot be understood without referring to certain anatomical peculiarities that do not exist in the adult. These characteristics depend on the absence of respiration, and disappear when it is established.
1st. The septum between the auricles of the heart is imperfect, having in its center a valvular oval aperture called the foramen ovale.
2d. The pulmonary artery, soon after its origin, gives off a branch, the ductus arteriosis, which enters the aorta just below the arch. The pulmonary arteries are very small.
3d. The umbilical artery in the fœtus is a large vascular trunk, which is nearly obliterated in after life. The two umbilical arteries run forwards and inwards along the lateral and superior parts of the bladder, then curve forwards to the abdominal wall, along which they ascend to the umbilicus, then pass along the cord to the placenta.
4th. The fœtus further differs from the adult in having an umbilical vein, which comes from the placental tissue, traverses the length of the cord, passes through the umbilical ring, is mostly distributed to the liver, but has a supplemental vein situated at the thick edge of the liver, and leading to the vena cava ascendens, called the ductus venosis.
The general effect of all these peculiarities is to render the heart virtually a single one; to provide for the quiescent state of the lungs, and to modify the distribution of fresh blood.
The course of the blood in the fœtus is as follows: The blood circulating in the umbilical vein is, on entering the fœtus, a part of it discharged through the ductus venosis into the vena cava; another part is distributed to the liver, and is brought to the vena cava by the hepatic veins, and then mingles also with that from the inferior extremities, and then with that from the upper extremities as it passes into the right auricle. A part of this is transmitted through the right ventricle, and thence (except a supply for the nourishment of the lungs) through the ductus arteriosis into the descending aorta. A second and larger part passes through the foramen ovale into the left auricle, then into the left ventricle and arch of the aorta, the branches of which supply the head and upper extremities. The continued stream passes into the descending aorta, mixing with that already described. The whole now descends to the lower part of the aorta, where a portion is sent to the inferior extremities, but a larger part is drawn into the umbilical arteries, and is carried by them into the placenta.
After birth remarkable changes take place. Something in the circumstances in which the child is placed stimulates respiration and crying, by which means the lungs are inflated, and space is afforded to the pulmonary circulation, which supercedes the use of the foramen ovale and ductus arteriosis; the blood from the lower extremities cannot pass through the umbilical arteries, and does pass through the ascending cava into the right auricle and ventricle, then into the lungs, where it undergoes analagous changes to those effected in the placenta, and is distributed to the body generally. The fœtal openings are generally obliterated in the course of a week, though the foramen ovale, or the ductus venosis, may continue pervious for two or three weeks; but soon the ductus venosis and the umbilical arteries are obliterated and the adult circulation established.