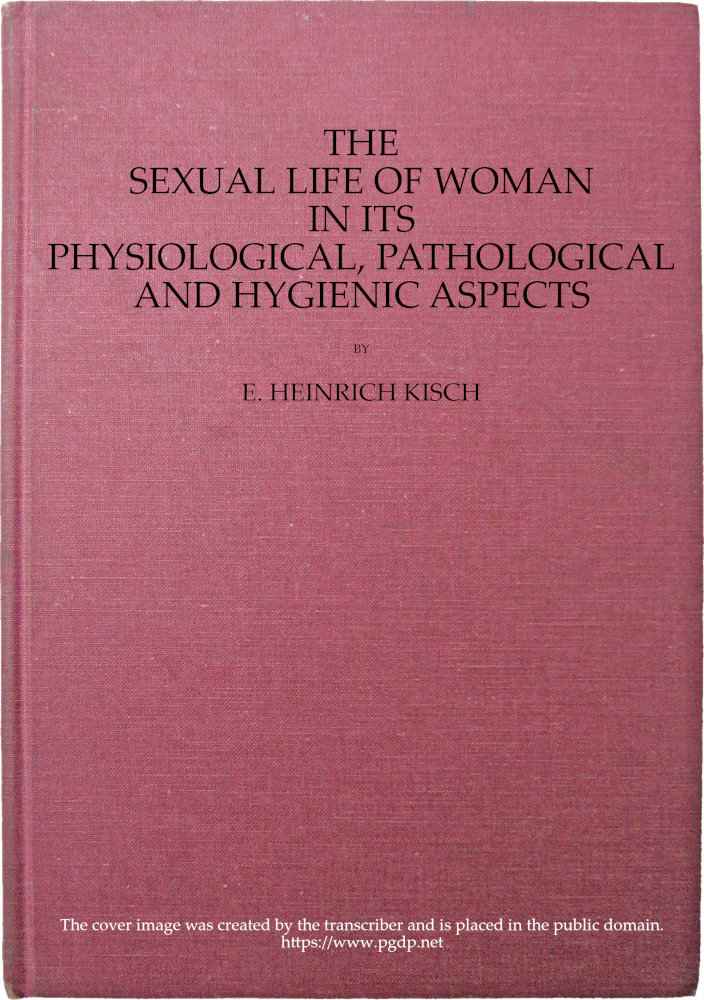
Fig. 47.—Horizontal section through the female breast. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
Thus it becomes comprehensible that even in healthy girls, the first appearance of the catamenia and likewise the expectation of the flow induce a certain modification and alteration in the whole nature and disposition. Girls often lose their previous cheerful and lively character, becoming quiet, self-absorbed, sometimes even melancholy; they are disinclined for study, have a repugnance to all sustained physical or mental activity, become annoyed and snappish on slight occasion, are restless at night, consider themselves to be ailing, and so on. During the first menstruation girls commonly appear pale and anxious, they have blue lines beneath the eyes, the face has a tired aspect, the movements lack energy, and a general want of tone combined with an abnormal irritability may be noticed. Some days before the first menstruation, the vulva, the labia majora and minora, and the vaginal mucous membrane, are swollen, the clitoris becomes conspicuous in consequence of erectile processes, a slight secretion appears in the genital passage, and the breasts become sensitive and slightly turgid. The urine deposits a thick sediment, and occasionally severe strangury is observed. In many cases, also, digestive disturbances occur, loss of appetite, constipation, or a tendency to diarrhœa.
The first menstruation usually lasts four or five days. On the first day the discharge is blood-stained mucus, thereafter becoming sanguineous. In some cases, the bleeding at the first menstruation is profuse and of long duration.
It is not always after the first menstruation that the subsequent discharges follow at the regular intervals of four weeks. In delicate, anæmic girls the second menstruation may not occur till several months have elapsed after the first; less often the second menstruation ensues a fortnight after the first, or even earlier.
At the time of the menarche the sexual impulse, which has hitherto been dormant, becomes strongly developed. It is evoked at this time of life by the anatomico-physiological changes undergone by the reproductive glands; the stimulus aroused by these processes in the ovary, being conducted to the brain, awakens passion. At the same time the observation of the growth of the hairy covering on the genital organs, the development of the breasts, and the appearance of menstruation, tend to arouse erotic presentiments. The reading of romances, conversations with female friends, and observation of the conduct of full-grown persons, convert these presentiments into clear ideas, and excite the impulse to the production of passionate sexual sensations, the sexual impulse. How far these stimuli arising from the reproductive apparatus are encouraged and accentuated, on the one hand, or repressed and diminished, on the other, depends on external impressions of various kinds. The environment is the determinant for the further transformation of the as yet undifferentiated sexual impulse into the fully-developed copulative and reproductive impulses.
In his work on the Physiology of Love, Mantegazza describes the yearning and stress of the awakening sexual life, arising out of the presentiments, hazy sensations, and impulses, which are felt in the very earliest period of the developmental phase known as puberty.
In general, in a young girl during the menarche, the sexual impulse manifests itself rather in the form of semi-conscious reverie, of platonic love. The adolescent girl exercises her imagination with the circumstances of her chaste love, her mind turns to this subject when in solitude, her mood is apt to become melancholy, and it is the perusal of equivocal novels, or the educational assistance of sexually experienced female friends, that transforms the sexual impulse to a vivid flame.
Some authors believe that a sign of the awakening of the sexual impulse when directed toward some particular man is a change of color on the part of the girl when she sees this individual or hears him spoken of. Palpitation of the heart comes on, the pulse is increased in frequency, the respiration also, and the voice fails. In this manner, it is asserted, Galen discovered the love of a Roman lady, Justa, for the dancer, Pylades.
The psychological reaction of the sexual impulse at the time of puberty manifests itself, as von Krafft-Ebing points out, in manifold ways, common to all of which, however, is the emotional state of the mind, and the need that the strange and new feelings now experienced should find some objective centre of interest. Such objective and emotional interests lie ready to hand in religion and poetry, both of which, after the period of sexual development is at an end, and the originally incomprehensible desires and impulses have received an explanation, continue to have intimate relations with the world of sexual experience. Any one who doubts this must be reminded of the frequency with which religious fanaticism makes its appearance at the time of puberty. No less influential is the sexual factor in the awakening of æsthetic feelings. This world of the ideal opens itself at the time when the development of the sexual processes begins. * * * The love of early youth, continues von Krafft-Ebing, has a romantic, idealizing tendency. In its first manifestations it is platonic, and willingly exercises itself in poetry and history. But as the sensibility awakens, the danger arises that this passion, with its idealizing power, will be transferred to persons of the opposite sex who in intellectual, physical, and social relations are by no means all that could be wished. Hence proceed misalliances, elopements, and seductions, with the entire tragedy of impassioned love, which conflicts with the dictates of morality and convention, and sometimes finds its bitter end in suicide or a double self-destruction. Love in which the senses play too prominent a part can never be a true and lasting love. For this reason, first love is as a rule very transitory, since it is in most cases no more than the first flare of passion. * * * Platonic love is a thing without existence, a self-deception, a false description of sexual sensations.
Bebel remarks that the number of suicides among women of the ages of sixteen to twenty-one years is an exceptionally large one, and he refers this chiefly to unsatisfied sexual impulse, unfortunate love, secret pregnancy, and to betrayal by men.
(Precocious and Retarded Menstrual Activity.)
By the term precocious menarche we understand the pathological state in which a typical, four-weekly, sanguineous discharge from the female genital organs sets in at an abnormally early age, and is to be regarded as a symptom of a premature sexual development. Very commonly such children with precocious menstruation and premature sexual development, exhibit a comparatively high body-weight, great development of fat, early dentition; they look older than their years; and they have genital organs that also develop very early, with hair on the pubes and in the axillæ; the labia majora and the breasts resemble those of full-grown women, and the pelvis also has the adult form. Commonly also the sexual impulse develops early, whilst, in other respects, the intellectual development lags behind the physical. It is most probably a primary hyperplasia of the ovaries that gives rise to precocious menstruation, the ovarian follicles ripening earlier than usual. Frequently other pathological processes are associated with this early sexual development, such as general lipomatosis, rachitis, and new growths of the ovaries. In several cases of this nature, early conception has also been observed. According to oriental tradition, Khadijah was married at the age of five years to the prophet Mohammed, who cohabited with her three years later.
Even if we except those cases in which in earliest infancy there is a sanguineous discharge from the vagina which remains, however, an isolated occurrence, or if repeated is repeated a few times only and at quite unequal intervals (cases in which the bleeding cannot be regarded as menstrual—such, for instance as were reported by Eröss of six new-born female infants in whom a sanguineous discharge from the vagina appeared three or four days after birth and lasted two to five days, the infants not remaining subsequently under observation),—numerous well-authenticated cases yet remain in which menstrual hæmorrhage was observed before the end of the first year of life. One case, even, is recorded by Bernard in which from the time of birth to the twelfth year menstruation with molimina occurred every month, lasting two days; from the twelfth to the fourteenth year menstruation ceased, recurring subsequently at irregular intervals.
In the recorded cases of such precocious menstruation the menstruation recurred as a rule at regular intervals of four weeks; only in quite exceptional cases were the intervals three to five months.
Some of the most striking and well-authenticated cases of precocious menstruation recorded in the recent literature of the subject are appended.
Observed by Combys: A girl aged 6 years and 2 months had the appearance of a girl aged 14 or 15; she was a brunette, 3′ 10½″ in height, with full, firm, rounded breasts, girth of chest 28⅓″, mons Veneris covered with hair, uterus normal on rectal examination, hymen intact; menstruation had occurred regularly since the second year of life. Mother and five sisters began to menstruate between the ages of twelve and fourteen. General condition good.
Case recorded by Diamant: A girl aged 6 years, weight 75 pounds, thighs, buttocks, and breasts developed like those of a sexually mature woman, axillæ and mons Veneris covered with hair. Menstruation began at the age of 2 and recurred regularly, the flow lasting 4 days.
Case recorded by Plyette: A girl with precocious physical development began to menstruate in the fourth year of life; menstruation continued regularly with the exception of two monthly periods, when vicarious epistaxis occurred.
From the collection made by Gebhard of the records of fifty-four cases of precocious menstruation, giving the first appearance and the type of menstruation, the development of the breasts, the other signs of premature sexual development, and any complications that may have been observed, we extract the age at which the first menstruation occurred. This was:
| In a new-born | infant in | 1 case. |
| At the age of | 2 weeks in | 1 case. |
| At the age of | 2 months in | 1 case. |
| At the age of | 3 months in | 1 case. |
| At the age of | 4 months in | 1 case. |
| At the age of | 5 months in | 1 case. |
| At the age of | 7 months in | 1 case. |
| At the age of | 9 months in | 4 cases. |
| At the age of | 10 months in | 2 cases. |
| At the age of | 12 months in | 5 cases. |
| At the age of | 15 months in | 1 case. |
| At the age of | 16 months in | 1 case. |
| At the age of | 18 months in | 2 cases. |
| At the age of | 19 months in | 1 case. |
| At the age of | 22 months in | 1 case. |
| At the age of | 2 years in | 4 cases. |
| At the age of | 2½ years in | 1 case. |
| At the age of | 2 years and 9 months in | 1 case. |
| At the age of | 3 years in | 6 cases. |
| At the age of | 3½ years in | 1 case. |
| At the age of | 4 years in | 4 cases. |
| At the age of | 4 years and 3 months in | 1 case. |
| At the age of | 5 years in | 1 case. |
| At the age of | 5½ years in | 1 case. |
| At the age of | 6 years in | 1 case. |
| At the age of | 6½ years in | 1 case. |
| At the age of | 7 years in | 3 cases. |
| At the age of | 9 years in | 2 cases. |
| At the age of | 11½ years in | 1 case. |
From this collection of Gebhard’s we learn that in one case menstruation already existed at birth, and that in a large number of cases it occurred before the expiration of the first year. In many cases the development of the breasts preceded the appearance of menstruation, and was noticed from the time of birth. The vulva also early exhibited the characteristics seen in the sexually mature woman. Further, a high body-weight, great development of fat, and early dentition, were usually seen in these cases, in which, however, the intellectual development was not in correspondence with that of the body.
In several of these cases of premature puberty, moreover, sexual intercourse and even parturition occurred at a very early age. A girl in whom menstruation began at the age of one year, gave birth to a child when she was ten years old (Montgomery). A girl who began to menstruate at the age of nine years, became pregnant very shortly afterward (d’Outreport). The well-known case recorded by Haller, in which at birth the pubic hair was already grown, and in which menstruation began at the age of two years, was also one of very early pregnancy, the girl giving birth to a child when nine years old. Another girl in whom at birth the pubes were already covered with hair began to menstruate when four years old, copulated regularly from the age of eight, and at nine years became pregnant, and was delivered of a vesicular mole with an embryo (Molitor). A girl began to menstruate at the age of two, had a growth of hair on the pubes and developed mammæ at the age of three, and became pregnant at the age of eight (Carus). With these cases must be classed that observed by Martin in America of a woman who was a grandmother at the age of twenty-six. Lantier, in his Travels in Greece, speaks of a mother of twenty-five with a daughter of thirteen.
Observations made by Kussmaul and by Hofmeier prove that in many cases changes in the ovaries form the probable cause of precocious menstruation and the other phenomena of premature puberty. In one case of Hofmeier’s, for instance, of a girl of five with precocious menstruation, the removal of a rapidly growing ovarian tumor was followed by the cessation of menstruation, and the pubic hair, which had been shaved off, did not grow again.
Abnormally early puberty related to the early practice of sexual intercourse is seen in many prostitutes. This is shown by the following figures relating to 150 prostitutes in Russia. Sexual intercourse began:
| In | 1 prostitute at the age of | 9 years. |
| In | 1 prostitute at the age of | 10 years. |
| In | 4 prostitutes at the age of | 12 years. |
| In | 12 prostitutes at the age of | 13 years. |
| In | 14 prostitutes at the age of | 14 years. |
| In | 33 prostitutes at the age of | 15 years. |
| In | 36 prostitutes at the age of | 16 years. |
Thus, among the 150 prostitutes, 65 were less than 16 years of age.
Parent-Duchatelet found among 3,517 prostitutes under official observation, 5.6 per cent. under 17 years of age. There were:
| 2 | prostitutes under 10 years of age. |
| 3 | prostitutes under 11 years of age. |
| 3 | prostitutes under 12 years of age. |
| 6 | prostitutes under 13 years of age. |
| 20 | prostitutes under 14 years of age. |
| 51 | prostitutes under 15 years of age. |
| 111 | prostitutes under 16 years of age. |
Martineau’s observations also showed that in nearly all prostitutes the first coitus took place in very early youth. Of 607 prostitutes there were 489 in whom defloration had occurred between the ages of 5 and 20 years. According to Grimmaldi and Gurrieri defloration usually takes place in prostitutes before they attain the age of 10 years.
Sometimes we find increased sexuality in early life as a pathological manifestation—psychopathia sexualis. Thus, Esquirol records the case of a little girl aged four years who undertook improper manipulations in association with little boys. A female prisoner, Lombroso writes, had at the age of six years practiced mutual masturbation with her brother aged seven, and at the age of eight years underwent defloration; another murderess, while still a schoolgirl, had conducted herself after the manner of an experienced prostitute. Laurent reports the case of a girl who from the age of ten was engaged in sexual malpractices with her brothers and sisters, and finally underwent defloration at the age of fifteen.
In many cases premature sexual development is manifested by enlargement of the breasts and growth of the axillary and pubic hair, and yet menstruation fails to appear. Thus, Kussmaul has observed girls who while yet children exhibited all the external characteristics of sexually mature women, but who had not yet begun to menstruate. Ploss has published a photograph showing in a girl five years of age the mons Veneris and the labia majora developed like those of a full-grown young woman, and covered with long thick hair; in this case, however, not only had menstruation not yet begun, but the breasts were still in the infantile condition.
The opposite state to menarche praecox is that in which the first appearance of menstruation is unduly delayed; it may be even till after the age of twenty. Such a postponement of the menarche sometimes occurs in girls who exhibit at this period of life an extraordinarily great general fatty development of the body, or a notably severe chlorotic state of the blood, or in whom during the years of development some sudden and extensive change in the mode of life has occurred, as for instance when the girl’s place of residence has been removed from the country to the town, or when she has had to undertake some completely new kind of physical or mental work. Raciborski attributes the late appearance of menstruation, at the ages of 20, 22, 24, or 26, in otherwise healthy girls, to an “apathy of the sexual sense,” a phrase which does not convey much meaning.
According to Marc d’Espine, puberty occurs early in girls with dark hair, grey eyes, a delicate white skin, and of a powerful build; late, on the other hand, in girls with chestnut hair, greenish eyes, a coarse darkly-pigmented skin, and of a delicate weakly build.
The genitals of girls in whom the first appearance of menstruation is delayed, frequently exhibit distinct signs of the backwardness of the reproductive organs in their development. The external genitals, in such cases, have little if any covering of hair, and are flabby and relaxed; the body and the fundus of the uterus are shorter and more slender than usual, the uterus as a whole is small and flaccid, sometimes anteflexed; the vaginal portion of the cervix is small, often almost undeveloped, its anterior lip barely projecting above the surface of the vaginal fornix; the vagina is usually short and narrow. The ovaries also are flaccid and inelastic, and occasionally are remarkably small. The breasts are small, the nipples and areolæ undeveloped.
In other cases, notwithstanding the delay in the appearance of the menarche, the genital apparatus is developed to a degree quite in correspondence with the age, but some pathological condition is present, for instance, the mucous membrane secretes excessively, exhibits a catarrhal tendency, there are erosions at the os uteri, etc.
Pathology of the Menarche.
A series of disturbances of function and pathological changes in the organs may occur at the time of the menarche, either directly connected with the genital organs, or etiologically dependent upon the changes occurring in these organs.
The commencement of menstruation, as we have already mentioned, may itself be abnormal in character, being either precocious (menarche precox), or retarded (menarche tardiva). But even where menstruation begins in a normal manner, the period of the menarche may be disturbed by a great number of pathological phenomena, of which the developmental processes occurring in the genital organs of the young girl must be regarded as the cause. First of all, the menstrual hæmorrhage itself may be abnormal in amount and duration. Then, again, functional disturbances of the most various character may occur: especially prominent are, disturbances of hæmatopoiesis, of the cardiac functions, and of the nervous system, and constitutional anomalies, which deserve attentive consideration; in addition we have to mention disorders of digestion and disorders of the sense-organs, among which latter certain changes in the skin especially deserve attention.
The diseases of the female genital organs at the time of the menarche are very various in nature. Whereas during infancy and early childhood the uterus and its annexa are in a state of complete quiescence, so that nothing occurs in them to attract attention, at the approach of puberty these organs emerge from obscurity, and the percentage of diseases of the reproductive organs suddenly rises to a great height. In very young girls, among diseases of these organs, we observe only malformations, malignant tumors, and gonorrhœal infections, and these pathological states, even, are quite rare; but at puberty all this is altered, and we have to do with disturbances of the menstrual function and their consequences, and with various inflammatory processes, and the period of sexual maturity offers us an overplus of diseases connected with the reproductive system, justifying the epigram of the French gynecologist who defined a sexually mature woman as “un uterus servi par des organes.”[20]
Anomalies of Menstruation.
Not infrequently, though the catamenial flow has appeared at the usual age and has for a time been regular, pathological disturbances of this function ensue.
Amenorrhœa at the time of the menarche may depend on complete aplasia of the ovaries, associated with a rudimentary and imperfect development of the uterus. In such girls, the development of whose reproductive system is thus imperfect, the continually expected menstrual flow fails to appear, in spite of the fact that a recurrent menstrual discomfort, evoked by the congestion of the genital organs, recurs at intervals of four weeks; as, for instance, colicky pains in the abdomen, irritable, nervous states, and mental disturbances. Further, amenorrhœa may be due to one of the various forms of atresia of the genital organs, as for instance to vaginal or hymeneal atresia. In such individuals the first period passes by without anything to attract attention. But at the second period, distress will usually be manifested; and from this time forward, painful contractions of the uterus will continue to occur at four-weekly intervals, and to become more violent as period succeeds period, whilst the menstrual discharge is wanting, or, to speak strictly, fails to find an outlet. The blood collects behind the seat of atresia, and the accumulation gives rise to pressure symptoms affecting the bladder and the rectum, and ultimately also the sacral nerves.
Menstruation, after its first appearance in normal fashion, may be suppressed in young girls in consequence of mental impressions, such as sudden fright; such cases are observed after an escape from a fire, or after a railway accident. Mental stimuli of less intensity but longer duration have a similar effect; sometimes these take the form of auto-suggestion. A well-known instance of the latter phenomenon is furnished by the case of a girl who, in consequence either of actual intercourse or it may be merely of too intimate an embrace with a man, fears she has become pregnant, and actually suffers from amenorrhœa though pregnancy does not really exist. I saw a case in which amenorrhœa was thus produced in a girl seventeen years of age, whose ideas on the process of sexual intercourse were still far from clear. She had permitted a young man to kiss her repeatedly and fervently, and to clasp her in a close embrace. She was then afraid that she had become pregnant; the catamenial flow, which had been regular since she was fifteen years old, ceased to appear; and it was not until at length I was consulted, was able to assure myself that the girl was essentially virgin, and was, therefore, in a position to reassure her as to her own condition, that menstruation again became regular.
Functional amenorrhœa may also occur in young girls in consequence of a sudden change in the conditions of life, a removal from town to country, for instance, or the reverse, travel in regions where the climatic conditions differ widely from those hitherto experienced, or a change from an active to a sedentary kind of occupation. Of this nature is the following case observed by Winter: Miss Q., aged 20; menstruation began at the age of 13 and was regular thereafter; on three successive occasions amenorrhœa occurred during a visit to Berlin, in one case lasting 3 months, another 2 months, and a third 6 weeks, whereas when at home menstruation was regular though somewhat scanty. There were no molimina. Examination showed the wall of the uterus to be thin, length of this organ 7 centimetres (2¾″), both ovaries distinctly palpable. Such a form of amenorrhœa as this, commonly disappears when the girl removes from the conditions unfavorable to the fulfilment of her sexual functions to the conditions favorable to that function.
Not infrequently a chill is in young girls the cause of suppression of the menstrual flow that has hitherto been quite regular, especially effective in this respect being, standing in cold water, getting the feet wet, the influence of rain and wind at the menstrual period on the insufficiently clothed lower extremities, and vaginal injections with water at too low a temperature. Such cases are common among the working classes, especially in washerwomen; but they are also observed among the well-to-do. An example is given by Winter: Miss H., aged 19; menstruation began at the age of 13, regular, at intervals of 4 weeks, the flow lasting 2 to 3 days, and being normal in amount. Several years ago the patient caught a severe cold through paddling in cold water during the period. Suppression of the menses resulted, amenorrhœa being complete for a year and a half. Then menstruation recommenced, but was irregular, sometimes anticipating, sometimes postponing the proper period, the interval being occasionally as long as four months; when it occurred, the flow was represented by a drop or two of blood only, and dysmenorrhœa was severe. At each proper period, if the flow failed to appear, severe molimina occurred in the form of abdominal cramps and headache. Examination showed the uterus to be normal in shape, 4½ centimetres (1¾″) in length, with a very thin wall; both ovaries were palpable, but smaller than normal.
The commonest form of amenorrhœa at this period of life is, however, the constitutional amenorrhœa associated with chlorosis. In chlorotic subjects we have to do, not with a symptomatic absence of the menstrual discharge, but with a failure of the ovarian function, the graafian follicles failing to ripen. We generally find, according to Gebhard, that chlorotic girls begin to menstruate at the usual age, or even earlier. Menstruation recurs once or twice at irregular intervals, and then gives place to complete amenorrhœa, it may be suddenly, it may be gradually, the flow on each occasion being scantier than before. In chlorotic patients, the menstrual discharge, when present, is very thin and watery, and often contains a large admixture of mucus derived from the cervical canal and the cavity of the uterus. The amenorrhœa may be of short duration; or it may last for a long time; so that it is not until after the lapse of months or years, and as a rule in consequence of suitable treatment, that menstruation recurs, being henceforward either normal in frequency and strength, or on the other hand permanently scanty and of the postponing type. The associated disorders from which the patients suffer take the form of headache, dizziness, syncope, feelings of oppression, disinclination for mental and physical exertion, and so on. Since in such cases the ripening of the ovarian follicles also fails to occur, when the amenorrhœa is complete the menstrual molimina are generally wanting (Gebhard).
Stephenson also states that in girls who have been chlorotic for a longer or a shorter time, menstruation frequently begins very early, in any case earlier than in healthy girls.
Usually in these cases various other disorders are associated with the amenorrhœa, such as colicky pains in the abdomen, sensitiveness of the abdominal wall to contact or pressure, headaches, attacks of hemicrania, general mental depression, and hysterical manifestations.
In chlorotic girls, at the times when menstruation is due, a watery discharge often occurs, sometimes slightly tinged with blood. Dysmenorrhœa may also occur at such times.
Attacks of menorrhagia in young girls are usually dependent on disturbances of the nervous system. Sometimes such an attack occurs at the very first menstrual period. Occasionally also menorrhagia may occur in association with chlorosis, to be distinguished according to Virchow from a rare condition named by him “menorrhagic chlorosis,” characterized by excessive menstruation of an anticipating type. The bleeding is in such cases seldom very profuse, however, but the periods are very long, and the intervals exceedingly short. Castan regards such profuse menorrhagia and metrorrhagia occurring in young chlorotic girls, especially at the commencement of puberty, as of an endoïnfective nature dependent upon auto-intoxication. The toxins lead to inflammatory and degenerative changes in the muscular substance of the uterus. According to Frænkel in these cases the ovaries are usually enlarged, seldom smaller than normal.
Frœlich has discussed this subject exhaustively in his monograph on Menorrhagia of Young Girls and Hypertrophy of the Cervix Uteri.[21] He states that the cases of menorrhagia in young girls at the time of the menarche may be arranged in two groups. In one of these the patients are chlorotic, and menstruation is normal neither in amount nor in duration, but it is the long continuance of the flow rather than its profuseness that gives rise to danger; in the cases belonging to the other group the patients are in excellent health at the commencement of puberty, but menstruation soon takes the form of long-continued and profuse menorrhagia. Cases of the latter kind are due to hypertrophy of the cervix uteri and fungous metritis. Such attacks of menorrhagia in young girls are seen also in cases of infectious disorders, as in smallpox, measles, scarlatina, and above all, influenza. The hæmorrhage often begins in the first days of the infection, and even during the period of incubation, one or two days before the appearance of the general symptoms. If the patient is attacked by influenza while menstruating, the menstrual flow may assume the character of a true menorrhagia. More often, however, in such cases, we have to do with an extra-menstrual hæmorrhage, such as may indeed be observed in girls who have not yet begun to menstruate.
Inflammatory Processes.
Chronic metro-endometritis, both corporal and cervical, occurs occasionally in young girls during the years of development. It is especially common in chlorotic subjects; and next to these in girls who are careless about the observance of hygienic precautionary measures during the menstruation. Thus it may result from physical exertion among the working classes; and from dancing, skating, riding, or mountaineering, among girls belonging to the well-to-do classes, during menstruation. Again, we meet with it in girls who work very hard at the sewing-machine; and, finally, in those who have long practiced masturbation. Through uncleanliness at the time of menstruation, the blood with which chemise and drawers are stained and the pubic hair soiled, undergoes decomposition, and this may lead to catarrhal inflammation of the vulva and vagina and of the endometrium. The most striking symptom in persons thus affected is the discharge of mucus, which in cervical metro-endometritis leads to a very moist condition of the external genitals, and leaves greenish-yellow spots on the under-linen; in corporal metro-endometritis the discharge is of a thinner consistence, milky in appearance, and not very abundant. As a result of the endometritis, the patient suffers from various pains in the body, a feeling of fulness, sacrache, general sense of fatigue, and diverse nervous manifestations; sometimes also from dysmenorrhœa, strangury, or obstinate constipation. In consequence of the great thickening of the mucous membrane that often occurs, menstruation becomes very profuse and long-continued, lasting from one to two weeks.
A form of chronic vulvitis, sometimes, though indeed quite rarely, met with in girls at this time of life, is inflammation of the external genitals dependent on masturbation. As characteristic signs of this we may observe an elongation of the nymphæ, the clitoris, or the præputium clitoridis, and at the same time on the inner surface of the greatly stretched labiæ we may notice a great increase in the sebaceous glands, so that the yellowish spots formed by these structures may be seen beneath the mucous membrane with the unassisted eye—the mucous surface, indeed, may be slightly uneven in consequence of their enlargement, so that they resemble small retention-cysts. The mucous membrane of the vulva between the margin of the hymen and the nymphæ is moreover, according to Veit’s description of masturbatory vulvitis, often beset with small pointed excrescences, the soft furrow between the clitoris and the external orifice of the urethra being very commonly marked by swelling of the mucous membrane and the presence of these little outgrowths; but sometimes also the parts lying to either side of the urethral orifice may exhibit similar changes. These small structures differ entirely from pointed condylomata—they do not branch, they occur only upon the vulval surface proper, not upon the parts exhibiting the characters of true skin, and they are non-infecting. More particularly, it must be remembered, we find these changes principally in virgins in whom on account of obscure symptoms an examination of the genital organs has been undertaken, and who suffer in addition from nervous and hysterical manifestations. The hymen, when intact, as it usually is in these cases, furnishes objective evidence that sexual intercourse is not the cause of the patient’s trouble, and indeed a distinctly ascertainable cause is hard to find. The patient usually exhibits abnormal sensitiveness and excessive prudery. Veit is of opinion that the association of all these symptoms justifies the diagnosis of masturbation as the exciting cause of the chronic vulvitis; in such cases we may at one time find the mucous membrane pale, but at a later examination fiery red, and we often see a clear, transparent secretion exuding from the ducts of Bartholin’s glands.
In consequence of long-continued masturbation, other pathological changes may take place in the female genital organs, such as hypertrophy of the nymphæ, proliferation or glandular hypertrophy of the uterine mucous membrane, ovarian irritation, pains in the ovarian region which, in severe attacks, may radiate to the thighs. These pains become more severe at the menstrual period, especially at the beginning of that period; and are sometimes also especially troublesome in the middle of the intermenstrual interval, in this case usually as a result of great bodily exertion.
These morbid processes in the genital organs of young girls have long attracted the attention of physicians, and it is more than sixty years since Bennet described the “virginal metritis” observed by him in twenty-three virgins. Bonton published in 1887 a monograph on this condition. Gallard assigns masturbation as its principal cause.
Retroflexion of the uterus is also sometimes observed in virgins, induced by the bad habits which are so common in young girls of retaining the urine for excessively long periods and of neglecting constipation. The prolonged distension of the bladder leads to a daily, long-continued stretching of the ligamentous apparatus of the uterus; the full bladder presses the uterus backwards, and after the viscus has been emptied, the flaccid ligaments are no longer able to restore the uterus to its normal position of anteflexion. The organ is left with its fundus directed backwards, and the intra-abdominal pressure keeps it permanently in this position; at the same time, an accumulation of fæces in the rectum, by pressing the cervix forward, favors this displacement of the uterus. Moreover, when the uterine tissues are flaccid through malnutrition in chlorotic or anæmic subjects, the organ yields more readily to mechanical influences than it would if its muscular tone was healthy.
Disorders of Hæmatopoiesis.
Chlorosis is in general rightly regarded as a disease of the period of puberty etiologically dependent on the processes that at this time of life occur in the genital organs. Its appearance generally coincides with the menarche, occurring at the age of 14 to 16, or even later, at the age of 19 to 21. As regards the composition of the blood in chlorosis, investigations have shown that its hæmoglobin-richness is always diminished; its specific gravity is proportionately lessened, but the specific gravity of the serum is normal. The erythrocytes are normal in number, or only slightly diminished; their shape is sometimes normal, sometimes, however, poikilocytosis is present. The leucocytes are generally normal both as regards number and form; myelocytes (Markzellen) are also described as present in the blood of chlorotic patients (Neusser, Hammerschlag, Gilbert, Weil); the blood-plates are normal in number, the alkalinity of the blood also normal, the isotonicity of the erythrocytes rather low.
The relation of chlorosis to the menarche is variously explained. Kahane, in his elaborate monograph on chlorosis, regards it as an independent disease belonging to the group of “disorders of vegetation” (Kundrat), one which “according to its essential nature is an expression of the disharmony that obtains between the congenitally inefficient hæmatopoietic apparatus and the demands made upon the feminine organism by the processes of puberty.”
An insufficiency of the hæmatopoietic organs as regards their functional capacity is believed by Kahane to be in the case of women so far physiological inasmuch as their blood is inferior to that of men in hæmoglobin-richness and corpuscular richness to the extent of about 10 per cent. In this way the predisposition of the female sex to chlorosis may perhaps be explained. A further fact which must be taken into consideration is the difference between the development undergone by the respective sexes at puberty. In the female sex, this development is quickly completed, and has the characteristics of a revolution; but in the male, the development is a more gradual one, and has the characteristics of an evolution.
F. A. Hoffmann also regards chlorosis as associated with the development of the uterus and the establishment of menstruation. It is possible that these processes exercise some reflex influence; but we must also remember that the chemical processes involved in the growth and maturation of the ovarian follicles are still insufficiently understood, and that it is quite possible that these too may have powerful and unaccustomed effects on the organism such as may well disturb metabolic processes of a somewhat unstable character.
Grawitz, who regards chlorosis as a vasomotor neurosis in which disturbances arise in the interchange of fluids between the tissues and the vessels, refers the appearance of chlorosis at puberty to the general disposition to disorder exhibited at this age by the vasomotor system.
Other authors consider chlorosis to be an ovarian auto-intoxication, believing that under certain conditions the ovaries give off into the organism certain poisons; or, on the other hand, supposing that a certain antitoxic function, normally possessed by the ovary, fails. Von Noorden, for instance, regards chlorosis as a disorder of blood formation referable to a disturbance of the internal secretion of the ovary during the developmental period.
Blondel, who also regards ovarian auto-intoxication as causal, is of opinion that chlorosis is induced by products of decomposition formed in the organism during the process of growth. As in childhood the thymus gland, so later in life the ovary, renders these products innocuous. When this peculiar functional activity of the ovary is retarded in its appearance, the intoxication effected by the products of decomposition formed during the process of growth gives rise to chlorosis.
Meinert, in an interesting manner, brings the harmfulness of wearing a corset during the years of development into etiological relations with chlorosis. In the transitional period between childhood and the age of puberty the wearing of the corset usually begins. Now Meinert discovered that in chlorosis, as a result of wearing a corset, a vertical or subvertical position of the stomach ensues as a partial manifestation of enteroptosis, leading to tension on the abdominal plexus of the sympathetic, which in turn results in changes in the blood, and other nervous symptoms. According to this view, chlorosis is a peculiar general neurosis dependent upon an artificially induced gastroptosis; this form of enteroptosis being due, not to relaxation of the suspensory ligaments of the abdominal viscera, but to pressure exercised by adjacent organs in consequence of a change in the form of the thorax, which has been permanently constricted by tight-lacing (fixierter Schnurthorax).
Of importance is the fact that in girls suffering from chlorosis a condition of hypoplasia of the genital organs is not infrequently met with. It would seem, not only that imperfect development of the female genital organs may be a cause of chlorotic changes in the blood, as appears possible in view of the relations between the ovaries and the hæmatopoietic organs through the intermediation of the sympathetic system; but also that genuine chlorosis and the anomalies of the genital organs met with in this disease, may perhaps be common manifestations of some more general disturbance.
According to Virchow, two distinct forms of chlorosis are to be recognized, one form in which no great abnormalities of the reproductive apparatus exist, and another form in which imperfections in the development of the central portion of the vascular system are associated with similar imperfections in the reproductive apparatus. In many cases of chlorosis, he found the ovaries small and imperfectly developed, in an infantile condition; in other cases, however, they were three times the normal size; the development of the uterus in such cases usually corresponds with that of the reproductive glands. With regard to the etiological connection between chlorosis and developmental disturbances, Virchow inclines to the view, that in chlorosis a predisposition, either congenital or else acquired in early youth, must be assumed to exist, but that this does not manifest itself by the production of actual disorder until the arrival of puberty; and he considers it likely that primary deficiencies of the blood and the vascular apparatus hinder the development of the reproductive apparatus.
Stieda found that in chlorotics displacements of the uterus were common, with abnormal narrowness of the vagina, absence of the pubic hair, imperfect development of the pelvis, and the growth of the breasts interfered with to this extent, that the nipples and areolæ were abnormally small. He classifies these manifestations as disturbances of development in the sense that they are among the so-called stigmata of degeneration. If in chlorotics the breasts in certain cases have a normally full and rounded appearance, this appearance is sometimes deceptive, the fulness being due, not to a proper growth of the parenchymatous mammary tissue, but to an excessive deposit of fat. Genuine chlorosis, therefore, not referable to some other primary disorder, is a developmental disorder, in the sense in which various other stigmata of degeneration met with in the human body are developmental disorders, and is indeed frequently associated with other stigmata of degeneration, or with malformations due to arrest of development, as for instance, an infantile type of pelvis or of genital organs, abnormalities of the cranial bones, vaulted palate, the root of the nose broad and depressed, extreme prognathism.
Hegar also maintains the view that chlorosis is in most cases a developmental disturbance, the origin of which is not limited to the so-called years of puberty; it often arises from noxious influences which are either strictly inherited or began to operate when the infant was still in her mother’s womb. Frænkel is inclined to regard a primary developmental disorder of the genital organs as the cause of many cases of chlorosis.
Recently, Breuer and Seiler have undertaken experiments on bitches, which they spayed at the outset of puberty, and from the results of these experiments it seems probable that a disordered influence exercised by the ovaries on the blood plays a part, at least, in the pathological mechanism by which chlorosis is induced.
The intimate relationship believed to exist between chlorosis and the sexual life of woman finds expression in the opinion, which dates back to the days of antiquity, and has been widely held even by physicians, that the disease (hence designated morbus virgineus or febris amatoria) is due to sexual abstinence in individuals with powerful sexual impulse, and that for this reason chlorosis is often cured by marriage. This result of marriage, which, though apparent merely, may indeed often be witnessed, is explained by Kahane on the ground, that in very many cases, the symptoms of chlorosis become less severe after the first five years have elapsed since the commencement of puberty, the improvement occurring quite independently of the marriage or continued celibacy of the sufferer. The influence of marriage in curing chlorosis is thus apparent merely to this extent, that a very common age for marriage in women is precisely in the twentieth, twenty-first, or twenty-second year, when five years have passed since menstruation began. By this time the organism will to a large extent have become accommodated to the demands made upon it by the processes of puberty. Experience also shows that chlorotic girls sometimes continue to suffer from the various symptoms of chlorosis even after they have become wives, and that chlorosis is not infrequently rendered more severe by the puerperium—but in a wife it is no longer customary to describe such symptoms by the name of chlorosis, they are called anæmia, hysteria, nervousness, etc. Further, in order to give the doctrine of morbus virgineus its death-stroke, Kahane directs attention to the fact that numerous cases of chlorosis are met with in young girls who are far from practicing sexual abstinence, especially, for instance, amongst the lower classes, amongst whom it is hardly customary to wait for marriage before beginning sexual intercourse. The connection between masturbation and chlorosis, which has also been widely alleged from the etiological standpoint, is moreover one that cannot be admitted. On the other hand it is easy to understand that the erotic reveries which are so often seen in chlorotic girls are very likely to induce the habit of masturbation.
In young girls at the time of the menarche, especially in those who suffer from amenorrhœa or from irregular menstruation, the anæmic form of obesity not infrequently develops. Such patients at the time of puberty exhibit signs of marked anæmia in association with a notable increase in fat. The skin in such cases is always strikingly pale and of a whitish-yellow color; in bodies which are in other respects beautiful the bust may have the appearance of a marble statue. Such girls are strikingly stout, but the fatty tissue is flaccid, soft, and spongy, and dependent parts readily become œdematous; the muscular system is generally feeble.
What especially characterises this anæmic form of lipomatosis in young girls is, that, even in mild forms of the affection, cardiac symptoms are apt to become prominent. Frequent and violent palpitation will occur even in the absence of any severe exertion or especial excitement, often also we see shortness of breath, precordial pain, anxiety, respiratory distress, and sensations of chilliness and fatigue.
The principal cause of the obesity in these cases is to be found in the anæmia, inasmuch as the diminution in the number of the erythrocytes is a diminution in the number of the oxygen-carriers, and this entails defective and insufficient oxidation. The deficiency in the albuminous constituents of the body also gives rise to a rapid and extensive deposit of fat, the power for the combustion of the fats absorbed from the food being insufficient. An auxiliary factor in producing obesity in such anæmic girls is their disinclination to physical exercise, dependent on the speedy onset of sensations of fatigue. The long-continued repose of the muscles, and the remaining almost continuously in close rooms insufficiently supplied with oxygen, also result in the withdrawal from the blood of the circulating fat and its deposit as adipose tissue.
Albuminuria at the time of the menarche is a disease of development which is not infrequently met with in chlorotic girls, as in adolescent boys. On examination of the urine in such young girls we detect the presence of a variable quantity of albumin, which is present especially after severe physical exertion, mental application, or emotional excitement, whilst the urine secreted at night is usually free from albumin. The skin is pale, the accessible mucous surfaces are comparatively colorless, the face is puffy, the eyelids are œdematous; the patients suffer from various nervous troubles, especially headache and dizziness, and they are also liable to dyspeptic disorders.
The cause of this albuminuria of puberty is according to von Leube in part disordered hæmatopoiesis, in part a slight degree of cardiac insufficiency with a tendency to stasis. At the time when the processes of development and the growth of the body in height are most active, there is not a corresponding increase in the energy of hæmatopoiesis, and the heart also fails to keep pace with the growth of the body and to meet the demands thus made upon it by vigorous growth and increased energy. In general the capacity of the heart in such individuals is indeed sufficient to maintain the circulation through the kidneys; but as soon as the functional activity of the heart is more strongly taxed and the energy of the circulation consequently declines, albuminuria occurs—and occurs all the more readily in consequence of the fact that, the hæmoglobin-richness of the blood having been lowered by the customary anæmia, the epithelium of the renal glomeruli is badly nourished and functionally inadequate.
When the period of the menarche is safely passed, when the menses recur with regularity, and the chlorotic manifestations disappear, when the process of hæmatopoiesis has improved in quality, and the growth of the body is completed—when, in short, the functional equilibrium of all the vital processes becomes re-established, the albuminuria of puberty ceases. It seems, however, that those who have suffered in this way are predisposed to a return of the albuminuria at the climacteric period, when the metabolic balance is once more disturbed.
Cardiac Disorders.
The commonest cardiac disorder at this period of life is nervous palpitation, occurring in young girls who are in other respects in good health, being free from anæmia and from any discoverable disease of the heart or vessels. That this disorder is dependent on the sexual processes is indicated by the fact that it first manifests itself in a stormy manner some time, weeks it may be or months, before the first appearance of menstruation; recurring at irregular intervals, the attacks continue till after the first menstruation, and cease soon after the regular return of the period. Objectively, the palpitation of the heart manifests itself by an increase in the frequency and strength of the cardiac impulse, and increased frequency and tension of the pulse; in a few cases, however, it is perceived subjectively only by the patient, as a distressing sensation of excessively frequent and powerful cardiac action. In the former group of cases, the enhanced activity of the heart is perceptible, not only by auscultation, by which we usually find the heart-sounds quite pure, but also by inspection, which shows us the violent agitation of the thoracic wall and increased pulsation of the carotids. On percussion, no change is found in the area of cardiac dulness. The frequency of the pulse is increased, usually reaching 120 to 140 beats per minute; it is full, and may be intermittent or irregular. In those cases in which the palpitation of the heart is a purely subjective sensation, we find no increase either in the frequency or in the strength of the pulse, which may indeed be less frequent than normal. With the palpitation is associated a sensation of strong pulsation in the great vessels of the neck, and often there is pain on the left side of the lower part of the chest, with a sensation of shortness of breath, respiratory distress, precordial pain, and a feeling of pressure upon the chest. Respiration is shallow, and abnormally frequent. The attacks of palpitation recur daily in some patients, in others at intervals of several days; they may occur entirely without exciting cause, or with a cause so trifling that it would not in a normal subject have produced any nervous excitement; the duration of the attacks varies from a few minutes to several hours, and they may occur either by day or by night; in the intervals between the attacks the functions of the heart and the arteries are conducted in a normal manner. The pulse-curves I have obtained during the attacks of palpitation, in those cases in which the manifestations were objective as well as subjective, exhibit a high pulse-wave, the upstroke being rapid and steep, the downstroke also sudden and steep, the predicrotic elevation but little marked, the dicrotic elevation often very distinct.
Less frequent than such attacks of palpitation recurring at irregular intervals are paroxysmal attacks of tachycardia, in which the frequency of the heart and pulse is increased to an enormous extent. This disorder manifests itself a little time before the first appearance of menstruation, thenceforward recurring regularly every three or four weeks, accompanying menstruation, or occurring at the proper menstrual period if menstruation is in abeyance; the attacks last several days. This trouble also disappears a few months after the establishment of menstruation.
Associated with these cardiac troubles are, not constantly indeed, but in the majority of cases, disturbances of the digestive organs.
From the heart-troubles already described, another group of cases must be distinguished, which are also observed at the time of the menarche. They occur in girls in whom the first appearance of menstruation is strikingly delayed, not having yet begun at the ages of 18, 19, or 20 years, or in whom considerable irregularities have occurred in connection with the commencement of menstruation. In such girls, in whom menstruation has appeared late and been irregular, or who are perhaps entirely amenorrhoeic, cardiac troubles may be so pronounced that the physician may be led to suspect the presence of organic disease of the heart. The most prominent symptom is frequent and violent palpitation, with strong pulsation in the carotids, respiratory distress, and feeling of anxiety, on continued exertion or even on very slight occasion. On percussion, the heart is not found to be enlarged; on auscultation, the heart-sounds are found to be very loud, often with a systolic murmur in the mitral region, whilst over the lower end of the internal jugular vein, the humming-top murmur (bruit de diable) is audible. The pulse is increased in frequency, at times arhythmical, and easily compressible. The sphygmographic tracing usually shows a subdicrotic or dicrotic character. The upstroke is not high; the downstroke descends low, almost to the lowest level of the curve, before the enlarged dicrotic elevation begins. The skin is always strikingly pale, pale also are the visible mucous surfaces, the hæmoglobin-richness and the corpuscular richness of the blood are considerably diminished, a feeling of fatigue and various other nervous manifestations are constantly present—in short, in all cases we have to do with the well-known chlorotic disposition, sometimes in association with the manifestations of the anæmic form of lipomatosis universalis. In several such cases, skin affections were also present. Some suffered from acne vulgaris of the face with the usual comedones; others perspired profusely from the palms of the hands and the soles of the feet; others exhibited a bluish coloration of the nose and the ears.
There is yet a third form of heart trouble, much rarer indeed than the forms already described, from which young girls sometimes suffer at the time of the menarche. It occurs in girls who just before the first appearance of menstruation have grown very rapidly, “shooting up to a great height.” They are not anæmic, nor do they appear “nervous;” but they are extremely thin, and they have grown enormously in height during the previous year. These individuals also, who in the previous course of their life have been free from heart trouble, now complain of cardiac distress. As in the cases previously described, they complain of severe palpitation, a feeling of fulness in the chest, shortness of breath on exertion, etc.; but the results of the objective examination are very different. The cardiac dulness is increased in area, especially in vertical extent, the apex-beat may be normal in position or displaced outwards, the impulse is always heaving, abnormally powerful and resistant, the heart-sounds, especially those of the left ventricle, are louder than usual, the aortic second sound accentuated, sometimes ringing, the carotids pulsate visibly. The radial pulse, the tension of which is abnormally high, can be compressed by the finger only with difficulty; sometimes it is jerky in character. The sphygmographic tracing shows a rapid and steep upstroke; in the downstroke, the predicrotic elevation is much larger than normal and also nearer the summit of the curve. Thus we see that all the signs of cardiac hypertrophy are present, hypertrophy, that is to say, of the left ventricle.
The cases of this nature that have come under my observation have not been in girls of the working classes, but among the well-to-do. We cannot therefore regard them as due to overstrain of the heart in consequence of excessive bodily exertions, comparable to the cases met with in young recruits after long marches and violent exercise. We must rather assume that the development of the female genital organs has evoked a storm in the cardio-vascular system, more especially that in some way an increased resistance has been offered to the work of the heart, and that thus the hypertrophy has been brought about; though we may suppose that other unfavorable influences have also been in operation. Such an influence, in these cases, is the rapid growth of the body, which makes enhanced demands on the work of the heart; another is furnished by the almost universally worn unhygienic article of clothing, the cuirass-like corset, which offers a rigid hindrance to the rapid growth of the female body, to the development of the breasts, the thorax, and the upper abdominal organs, and which fails to accommodate itself to the changing conditions of growth, so that much extra work is thrown upon the heart. In such young girls we have very frequently found tight stays, which were worn unchanged without regard to the growth of the body in length, and which, by pressure on the epigastric region, elevation of the diaphragm, and limitation of the respiratory movements of the thorax, actually offered such considerable resistances to the driving power of the heart, as ultimately to lead to hypertrophy of the cardiac muscle.
Summing up our observations, we find that at the time of the menarche cardiac disorders occur in young girls which may be arranged in three groups of cases:
1. Nervous palpitation and paroxysmal tachycardia in persons in other respects in good health, the affection appearing shortly before the commencement of menstruation, and disappearing soon after the flow is regularly established.
2. Cardiac disorders occurring in young girls suffering from chlorosis, which itself results from the processes of the menarche.
3. Cardiac hypertrophy developing at the time of the menarche, and dependent on the circulatory disturbances associated with that process, its appearance being favored also by rapid growth of the girl and by unsuitable clothing (tight lacing).
With respect to the activity of the heart and the circulation of the blood at the time of the menarche, the little-known observations made by Beneke, on the growth of the heart and arteries in the various stages of development, deserve especial attention. According to this writer, the growth of the heart is slow until the age of fifteen years is attained, but becomes accelerated at the commencement of puberty. During this time of puberty, the blood-pressure attains its highest level, being comparatively low in childhood and later in life. The development at puberty of the female heart is less extensive than that of the male heart, and for this reason throughout adult life the capacity of a woman’s heart is on the average 25 to 30 cubic centimeters (1.5 to 1.8 cubic inches) less than that of a man. In women, also, the great arteries are on the average somewhat smaller than in men. The various arteries do not develop with equal rapidity throughout the period of growth; after puberty the common carotid grows very much more slowly than the common iliac artery, the former vessel being the only large trunk which has already nearly reached its maximum size at puberty.
The comparatively great development which the heart undergoes at the time of puberty is a phenomenon so important alike in its physiological and its pathological relations that it deserves the special designation of the puberal development of the heart; the commencement and the completion of puberty appear beyond question to be to a large extent dependent upon this development of the heart and upon the simultaneous rise in the blood-pressure of the systemic circulation due to the comparative diminution in the calibre of the arteries.
In the literature of this subject of cardiac disorders during the menarche, we find only short annotations on palpitation of the heart in young adolescent girls, and on cardiac manifestations in chlorotic subjects. Further, the statistical fact that valvular lesions of the heart are commoner in women than in men is by many authors explained on the ground that the disturbances of the time of puberty, which certainly occur more frequently and are more severe in the female sex than in the male, play an important part in their causation. Changes also in the vessel, such as cirsoid aneurysm (angioma arteriale racemosum), are supposed to be connected with the sexual processes of this period of life. C. Heine maintains that in consequence of puberty and of the sexual functions that become established at this period, a telangiectases will not infrequently undergo transformation into a cirsoid aneurysm; especially in cases in which menstruation is scanty and irregular, angiectatic tumors may exhibit a vicarious periodic increase.
Krieger describes nervous palpitation and also “cramps of the heart”[22] as occurring in girls who have not yet begun to menstruate, in the form of prodromal manifestations; similar attacks may occur also at every menstrual period in girls in whom menstruation is fully established. In most of these cases the pulse is increased in the patients who complain of a sensation of anxiety, and speak of feeling the heart roll, tremble, or flutter, to which is sometimes superadded a sensation of sudden cessation in its activity. Not infrequently there is a blowing adventitious sound, masking or accompanying the heart-sounds; there are also venous murmurs, especially when the heart-trouble is associated with anæmia or chlorosis. Of the cases of pseudo-angina pectoris[22] observed by Krieger, the attacks occurred as prodromal manifestations before the first appearance of menstruation in 22 per cent. of the cases, after menstruation was fully established in 78 per cent. of the cases; as regards the relation of the attacks, in cases of the latter group, to the menstrual period, they occurred before the flow in 33 per cent., during the flow in 67 per cent.; menstruation was irregular in 10 per cent. of the cases under observation, in most of the other cases menstruation had been irregular, but was now regular.
Hennig records a case in which he observed as a prodromal symptom before the establishment of menstruation the regular recurrence of congestion of the pelvic organs associated with cardiac disorder.
Diseases of the Nervous System.
The extensive transformatory processes occurring in the genital organs of young girls at the time of the menarche, and the powerful impression which the new thoughts, hopes, and fears excited at this period of life cannot fail to exercise on the nervous and emotional life, will enable us to understand how it is that the appearance of the first menstruation may give rise, especially in neurasthenic or psychopathic subjects, to manifold nervous disturbances and also to disorders of the mind.
Amongst the severe neuroses and psychoses liable to occur at the menarche in those suffering from congenital nervous weakness, in those the conditions of whose life are very unfavorable, and in those affected by some sudden disagreeable and powerful influences, we may enumerate: Hemicrania, precordial pain, hysteria, and epilepsy; impulsive manifestations, such as bulimia, longings for various unsuitable things, kleptomania, and pyromania; severe feelings of anxiety; various forms of psychoses.
On the other hand, the first appearance of menstruation has sometimes a favorable influence in girls suffering from nervous or mental disorder. This is seen, for example, in cases of chorea in fully developed, rapidly growing girls who have not yet begun to menstruate; in such subjects the chorea sometimes disappears as soon as menstruation is regularly established.
Quite frequently, the first appearance of hemicrania in young girls coincides with the menarche. According to Warner, hemicrania made its first appearance:
| In | 1 girl of | 3 to | 4 years. |
| In | 2 girls of | 5 to | 6 years. |
| In | 1 girl of | 6 to | 7 years. |
| In | 5 girls of | 8 to | 9 years. |
| In | 5 girls of | 9 to | 10 years. |
| In | 4 girls of | 10 to | 11 years. |
| In | 2 girls of | 11 to | 12 years. |
| In | 4 girls of | 12 to | 13 years. |
| In | 15 girls of | 13 to | 15 years. |
Toothache, according to Holländer, in the early days of puberty sometimes exhibits the twenty-eight-day type of menstruation. The same periodicity has been recorded in cases of vicarious bleeding from the gums in girls suffering from disturbance of the menstrual function.
In the period of the menarche and before this period, chorea minor occurs, as a functional disturbance of the motor region of the nervous system, and especially in girls is it associated with the processes of the period of physical development. The statistical data supplied by a number of authors, Hughes, Pye-Smith, Russ, Sée, and Steiner, show that the proportion of boys to girls affected with chorea minor is 1 to 2.8, and that of all ages 49 per cent. of the cases occurred at the ages of 6 to 11 years, 29.8 per cent. at the ages of 11 to 13 years. In several cases, in quite young girls suffering from chorea, pathological changes were found in the genital organs. Thus, in 24 out of 27 girls from the age of 9 to 15 years affected with chorea, Marie found the symptom-complex designated by Charcot as ovarie. Ovarian tenderness was manifested on palpation, and always on that side on which the chorea had first manifested itself. Leonard found in a girl aged eleven suffering from chorea, adhesion of the præputium clitoridis; after the separation of the prepuce, the chorea disappeared.